
Believe it or not, there are times when I'm unsure whether or not I should say something. Yes, shocking, I know but really, there are situtaions in my life where I have to wonder whether opening my mouth is going to be WORTH the outcome. Usually, yes, it is because I don't care if people don't like me for the fact that I share information (fact based, scientifically supported information). A favorite quote of mine:
"No one can make you feel inferior without your consent." -Eleanor Roosevelt
It is *so* true. You can't feel guilty because someone tells you that there is information that PROVES that breastfeeding is a superior infant choice unless you LET that make you feel guilty...and why on earth would you? Because you'd rather NOT know so that you can CHOOSE not to do it? I'm not sure, I honestly can't imagine (and remember, I have done it all and formula fed my other children, but when I learned more, I didn't feel guilty and start a mommy war, I took that information and did better). And this is, of course, just an example. Obviously formula exists for a reason and I would love to see it improved, regulated more strictly and, of course, for more breastfeeding information/support/breastmilk donors/etc were available.
But this is taking us FAR away from the point of my blogpost. :)
Sadly, you'd think the only things parents would argue about would be infant feeding, discipline, perhaps toys/devices and maybe sleeping arrangements. You might be surprised to know that another hot button issue in the momosphere is carseats. Yea, carseats. And not just the "Evenflo vs. Graco" type debate but people who ACTUALLY get offended when you tell them the LAW on infant/child carseats/restraints. (For carseat laws go here This lists the most basic information and needs to be read carefull and should also be cross-referenced. Also remember that MINIMUMS aren't the safest.)
While at Target this weekend, a woman was pushing her cart in front of me. She had with her a toddler and an infant, perched on the cart in his infant carrier. The straps on the carrier were so loose they were sagging, hanging off his shoulders and the chest clip was down by his groin. Now, it is likely she loosened this and pushed the clip down as soon as she got him out of the car (although that's a little scary too, considering he was teetering on top of the cart...) but I couldn't help but wonder, "What if he was in the car like that? What if she doesn't know (or worse, doesn't care) that it's incredibly dangerous?" and as I followed her (incidentally, we were just taking the same route through Target for about 5 mintues) I just couldn't muster up something to say to her. I didn't want to come off as rude, know-it-all, condescending etc. Part of my problem was trying to figure out HOW to say something to her. What would I start with? How would I broach that topic without her feeling totally defensive or insulted. And that wasn't my intention, by any means. And so, I contemplated so long that she took a different turn and then, it was too late. Still kicking myself for that one.
And what would have happened? Likely, she would have either told me she loosened it as soon as they got out of the car; told me to f*ck off and mind my own business (ouch); thanked me for my concern or said she didn't know and (hopefully) put it in effect. I sadly must admit I let that second possibility affect me too much and for whatever reason, I let it make me a bit nervous.
Hopefully next time I won't let my nerves get the better of me, after all, it really was a matter of life and death if her infant was riding in the car restrained (I use the term loosely) like that. And so my question to all of you fellow mommies is this:
What would you do in this situation and have you ever been in a similar situation where you felt compelled to say something? Did you? How did that go?
I think this could be a great discussion and, of course, needs to be kept civil and respectful. So sound off!
9.30.2010
Weaning is such sweet sorrow...
 When I was pregnant with my third child, Alex, I had set my mind on breastfeeding. I knew that my lack of success with my other two children was due to a lack of knowledge on breastfeeding. After all, just because it's natural doesn't mean it comes to you (or your baby) naturally. Yes, all babies are born with the basic need, tools, and know-how to breastfeed, but there is a lot of interference at play in today's maternity wards, and it can and does affect breastfeeding.
When I was pregnant with my third child, Alex, I had set my mind on breastfeeding. I knew that my lack of success with my other two children was due to a lack of knowledge on breastfeeding. After all, just because it's natural doesn't mean it comes to you (or your baby) naturally. Yes, all babies are born with the basic need, tools, and know-how to breastfeed, but there is a lot of interference at play in today's maternity wards, and it can and does affect breastfeeding.I figured in order to have an enjoyable and successful breastfeeding relationship this time around, I would need to arm myself with some basic understanding of what makes a good nursing relationship. Most women will tell you that the first few weeks are tough, but after that, it's smooth sailing. But many times, "tough" doesn't even begin to describe those first few weeks of nursing, as I experienced with baby #1.
My first source was nursing forums on the web, like different breastfeeding groups on the mothering site Cafemom.com. I learned a lot from these women, but many of them didn't seem to be too hell bent on nursing. There were many posts on weaning for convenience, supplementing, and bad advice that even I, as a so far unsuccessful nursing mother, noticed was bad. I was lucky enough to get a copy of "The Womanly Art of Breastfeeding" (a new edition has just recently been released with more updated information and witty writing style). This book was GREAT. I feel I owe my breastfeeding relationship with Alex to La Leche League. I read every chapter in that book that would pertain to the beginning of my nursing relationship.
At the moment of Alexander's birth in to this world, I accepted him on to my chest. We gazed in to each other's eyes and I attempted to latch him on the breast. Nope, he didn't want anything to do with it. However, after a little time had passed, he eagerly found his way and latched on. But I popped him right off.
One thing I had learned was my cracked, bleeding nipples with my first child, Maggie, were *not* normal and could have been avoided. Pacifiers and a lack of knowledge on how a baby SHOULD latch led to me suffering because of her poor, shallow latching during nursing. When Alex began his first breastfeeding, he was doing it wrong. I removed him from the breast, and we attempted again. As we would continue to breastfeed over the next few days, I continued to correct his latch when it wasn't perfect. I knew how to and what to look for, because I had made sure to learn before hand. It's hard enough adjusting to a new baby, much less a new baby and two toddlers *and* learning how to breastfeed! Having the information before all that stress made this whole nursing thing a ton easier.
Once we settled in to it, our nursing relationship took off. I knew I was going to breastfeed, but I was so happy to have been able to make it that much easier. My plan was to let Alex nurse until he weaned, an age that varies widely across the globe, and even across the country. Most children in the US wean between ages 2-3, but it's hard to tell as extended or "full-term' nursing isn't very common (or accepted) in the US and many women feel societal pressures to wean, even before the recommended and encouraged age of 1.
I must admit, I really didn't think he would nurse past 2. Age 2 was my goal. It is the minimum recommendation from the World Health Organization and the benefits of breastmilk don't stop...ever. I knew his health, and mine, would be optimal for as long as he continued to nurse. But again, I didn't know exactly how long that was going to last.
His 2nd birthday came and went, and "nursies" were one of his favorite past-times. I was happy to continue nursing, afterall, he was hardly sick and suffered no ear infections in his first 2 years of life.
Around age 2.5 I started to encourage and enforce certain rules. If he threw a fit, demanded to nurse, or pulled at my shirt, he was not going to nurse. He would have to wait. If the fit continued, he was not getting it. Just as with anything else, I disciplined him for bad or inappropriate behavior and his attitude toward nursing was no different. I also attempted to night wean him, as I noticed he was losing his suckling reflex (a sign that your child may be ready to wean) and it was getting painful to nurse at night.
I was not at all prepared for him to stop all together, and even these attempts at "regulating" breastfeeding were hardly successful, though I didn't give in or up.
Around the age of 2 years and 10 months my friend was visiting. Alex announced to her that he "had nursies for the last time.". It was so matter of fact and we both laughed at how funny the statement was. He responded with "Yup, I'm a big boy now.". At that moment in time, I did not believe anything he had said. He had been going to bed without nursing, and was maybe nursing once at night, but he still asked during the day. Some days it was only once or twice, others it seemed much more than that, but it didn't seem near done.
Sure enough, that *was* the end of it. As much as I was feeling ready for it to be over, I was surprised at how I felt once it WAS over. I think, in part, because I had expected to know the last time he was nursing, to remember it. To end the last 3 years with some sort of big "Hoorah!". But no, he had decided he was done. Perhaps, in part, to my gentle encouragement that we needed to go about things a little differently.
I do miss it every now and again, just because the bond was so wonderful and we were able to make that quiet, calm connection in the middle of a hectic day, but all in all, I am happy. It seems a little odd now, to have had this relationship for so long and now it's gone. He has become quite the snuggle bunny. I love it, because now we can just cuddle and he doesn't decide to start demanding to nurse, as if that was all I was good for. Instead, I get hugs, kisses, "I love you, mommy".
Yes, it's sad to think he has nursed for the last time, and I don't even know when that was, but I really like this "new" relationship. I hope that by nursing him until he and I were both done has served him well. I'm happy to have made such a turn around and he has taught me so much about mothering. Now, I can look forward to continuing to grow in our relationship, and to nursing the next baby until he/she is "a big boy or girl". :)
6.01.2010
I Am a Human Toilet: Repost
This is a blog I wrote back in 2008. I find it funny, reading it over again but the reason it's even on my mind is that I get the most RANDOM "ads" posted on it. I reject them all but some of the stuff is really weird (like, freaky weird). I'm debating deleting the originally blog so I don't have to moderate anymore inappropriate ads but until I decide for sure, I thought I'd share it here.
Enjoy :)
Being a mother comes with many other titles. You learn them as you go. You become a homemaker many times, a chef, a designer, a manager, a hostage negotiator, and many more things! One title I never thought I'd bear was that of "human toilet" but alas, my fate has been sealed...
I was first introduced to my new job duty with my first child. I was still breastfeeding Maggie and so she was having that seedy, mustard looking poopy as she wasn't on solids or anything yet. Well, I was a young, single mommy and we shared a room at my mother's, so I didn't have a nursery and I usually just changed her on my bed. As I carefully removed her poopy diaper and folded it ever so nicely, I figured she'd be fine diaper free for a sec (after all, it was all in the diaper, right?). Well, I wasn't prepared for what happened next! As I lifted her legs up to put her new diaper on, she projectile pooped ALL OVER ME! I was not only a new mommy, I was a young mommy, so this was not something I was AT ALL prepared for!! I was covered in seedy, liquidy poop! I changed clothes, sheets and finally her diaper and jumped into the longest, steamiest shower ever!
Now that I had experienced this, I knew you were never safe, not even for a moment, from the poop factor! I was always prepared with a fresh diaper to slip right now after the dirty one. I would even make sure to unfold it and prepare the tabs prior to removal of the soiled dipe!
I made it 5 whole years without ever experiencing a poop drench again! That is, until last night...
The baby beast was sitting on my lap, bouncing and cooing about, when I heard the puttering warning sounds of diaper doody (yes, that's a purposeful typo). As he ever so joyfully filled his drawers, my brother and I continued our conversation, that is until I felt wet...very wet. I figured he probably leaked a little and so I lifted him up and O.M.G. I was COVERED in his poopsie! I had no clue how it had made it's way from his bowels to my pants (and shirt, and chair...) because he had not a "drop" on him!!
I laid him down and went to clean up (I've learned now having 3 kids, that hot steamy shower I had the first time...was the last in a LONG time...). Once clean and changed I came back to solve this mystery. The beast was kicking around and laughing, not even phased by the mess in his drawers, but there was still no apparent leak!
Upon further examination, it was clear where the mess had seeped from. Somehow, and without leaving much of a mark, it had leaked out from between his legs, the crotch area, and nicely settled on moi. When I opened his diaper, there was barely a skidmark inside. He had, in fact, covered me in all of his wonderful poopiness.
I finally came to terms with the fact that on top of being a program organizer, a maid, a magician and a performer, I was also a human toilet.
Enjoy :)
2.26.2008
I am a human toilet.
I was first introduced to my new job duty with my first child. I was still breastfeeding Maggie and so she was having that seedy, mustard looking poopy as she wasn't on solids or anything yet. Well, I was a young, single mommy and we shared a room at my mother's, so I didn't have a nursery and I usually just changed her on my bed. As I carefully removed her poopy diaper and folded it ever so nicely, I figured she'd be fine diaper free for a sec (after all, it was all in the diaper, right?). Well, I wasn't prepared for what happened next! As I lifted her legs up to put her new diaper on, she projectile pooped ALL OVER ME! I was not only a new mommy, I was a young mommy, so this was not something I was AT ALL prepared for!! I was covered in seedy, liquidy poop! I changed clothes, sheets and finally her diaper and jumped into the longest, steamiest shower ever!
Now that I had experienced this, I knew you were never safe, not even for a moment, from the poop factor! I was always prepared with a fresh diaper to slip right now after the dirty one. I would even make sure to unfold it and prepare the tabs prior to removal of the soiled dipe!
I made it 5 whole years without ever experiencing a poop drench again! That is, until last night...
The baby beast was sitting on my lap, bouncing and cooing about, when I heard the puttering warning sounds of diaper doody (yes, that's a purposeful typo). As he ever so joyfully filled his drawers, my brother and I continued our conversation, that is until I felt wet...very wet. I figured he probably leaked a little and so I lifted him up and O.M.G. I was COVERED in his poopsie! I had no clue how it had made it's way from his bowels to my pants (and shirt, and chair...) because he had not a "drop" on him!!
I laid him down and went to clean up (I've learned now having 3 kids, that hot steamy shower I had the first time...was the last in a LONG time...). Once clean and changed I came back to solve this mystery. The beast was kicking around and laughing, not even phased by the mess in his drawers, but there was still no apparent leak!
Upon further examination, it was clear where the mess had seeped from. Somehow, and without leaving much of a mark, it had leaked out from between his legs, the crotch area, and nicely settled on moi. When I opened his diaper, there was barely a skidmark inside. He had, in fact, covered me in all of his wonderful poopiness.
I finally came to terms with the fact that on top of being a program organizer, a maid, a magician and a performer, I was also a human toilet.
5.14.2010
Setting Boundaries
I love the *idea* of letting my children explore and experiment with things, permitting they are appropriate and safe. However, I find that the *idea* of letting them do this and the reality of being able to allow it often collide...and explode.
I wish I could allow them to be crafty and NOT CARE that there was glue and glitter and marker all over the kitchen, but I have a house full of 7 people to maintain...plus, who wants to waste money replacing things that get damaged?
I wish I could laugh as they chased each other around the house, SHRIEKING with delight and making my ear drums ring, but, unfortunately, I do not enjoy migraines...plus you can only take so much medication before you're doing more harm than good!
I wish I could let them get FILTHY in the dirt playing outside, catching bugs and picking their nose, but I can't help but tell them to "Keep away from there, in case there's black widows!" or " Please keep those DIRTY fingers out of your mouth...and your sister's!"...plus, I really like to avoid unnecessary exposure to germs and deadly pests, even if SOME germs are a good thing.
I wish I could NEVER have to yell or raise my voice at my children, but if I never did they'd never hear me over their own chorus of cheers, chants and tears...plus, I hear yelling a little keeps you from going off the deep end completely.
I wish that I could say I loved breastfeeding ALL the time because it's only beautiful and wonderful and joyous, but then I'd be not only a liar but discrediting myself and the other moms when they are going through a BAD or DIFFICULT phase...plus, let's face it, after 2.5 years sometimes you just want to say no, because you can.
I wish that I could let my house stay in a constant state of toy mess and not get frustrated at the massive piles of trucks, barbies and stubbed toes that result from it but, I enjoy NOT stubbing my toe to a bloody nubbin and having a neat and organized house that doesn't automatically scream "KIDS LIVE HERE" when someone walks in the door...plus, who really enjoys having bloody nubs for toes?
I really do wish I could live up to the *idea* of that kind of mom, but instead, I'll keep doing my best to reach that point and not cry if I miss it by an inch...or a mile...plus, who REALLY wants to be *perfect* anyhow?
I wish I could allow them to be crafty and NOT CARE that there was glue and glitter and marker all over the kitchen, but I have a house full of 7 people to maintain...plus, who wants to waste money replacing things that get damaged?
I wish I could laugh as they chased each other around the house, SHRIEKING with delight and making my ear drums ring, but, unfortunately, I do not enjoy migraines...plus you can only take so much medication before you're doing more harm than good!
I wish I could let them get FILTHY in the dirt playing outside, catching bugs and picking their nose, but I can't help but tell them to "Keep away from there, in case there's black widows!" or " Please keep those DIRTY fingers out of your mouth...and your sister's!"...plus, I really like to avoid unnecessary exposure to germs and deadly pests, even if SOME germs are a good thing.
I wish I could NEVER have to yell or raise my voice at my children, but if I never did they'd never hear me over their own chorus of cheers, chants and tears...plus, I hear yelling a little keeps you from going off the deep end completely.
I wish that I could say I loved breastfeeding ALL the time because it's only beautiful and wonderful and joyous, but then I'd be not only a liar but discrediting myself and the other moms when they are going through a BAD or DIFFICULT phase...plus, let's face it, after 2.5 years sometimes you just want to say no, because you can.
I wish that I could let my house stay in a constant state of toy mess and not get frustrated at the massive piles of trucks, barbies and stubbed toes that result from it but, I enjoy NOT stubbing my toe to a bloody nubbin and having a neat and organized house that doesn't automatically scream "KIDS LIVE HERE" when someone walks in the door...plus, who really enjoys having bloody nubs for toes?
I really do wish I could live up to the *idea* of that kind of mom, but instead, I'll keep doing my best to reach that point and not cry if I miss it by an inch...or a mile...plus, who REALLY wants to be *perfect* anyhow?
5.11.2010
Placenta Encapsulation-Phase 2
I posted the first part of the process yesterday and I really hope you learned something you didn't know about placentas and encapsulation of them. After going through this process now, I am eager and excited to help another mama out by offering encapsulation for her. I hope this was useful to you and please, feel free to share this blog with mother's you know to spread the word on the benefits of placenta pills and help someone learn the process.

STEP 11:
After removing the placenta from the oven and letting cool, break larger pieces by snapping them. Pieces should be about 3/4 in.


STEP 12:

Place pieces in grinder (Mr. Coffee works great, but remember, you must only use this grinder for placentas so you'll need one separate from your "regular" coffee grinder). Note that some pieces may not grind down. Larger calcifications or clusters of hardened vessels will simply stay intact, that's ok. Just discard this larger chunks.
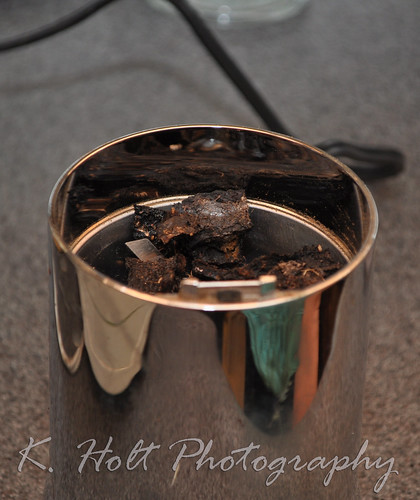
Your ground placenta should look like this:

STEP 13:
Pour all the ground placenta into a bowl or onto a deep plate.

STEP 14:

Take the two parts of your capsules (we used organic vegetarian gelatin capsules, sizes 0 and 00. 0 seemed to work best for me and is a little smaller.) and scoop them towards each other in the freshly ground powder, making sure to seal tightly. Place in "resting place" on paper towel.


STEP 15:
Discard any excess capsules that came in contact with the powder as well as any excess powder that you couldn't encapsulate.

STEP 16:
Wipe down the pills to remove any loose powder, grooved paper towels work great. Then place in jar/bottle/bag to give to mama. Store in fridge or freezer.

We were able to yield 122 good size capsules from this placenta. Mom takes about 3 tablets 2-3 times daily for general use or up to 8 a day if using to stave off post partum depression.

A huge thank you to the lovely Jessica J. for teaching Doula Faye and myself this art of placenta encapsulating. I am happy to offer this service to anyone who might be interested and we'd love to spread the knowledge, know-how and fun of this ancient art.
STEP 11:
After removing the placenta from the oven and letting cool, break larger pieces by snapping them. Pieces should be about 3/4 in.
STEP 12:
Place pieces in grinder (Mr. Coffee works great, but remember, you must only use this grinder for placentas so you'll need one separate from your "regular" coffee grinder). Note that some pieces may not grind down. Larger calcifications or clusters of hardened vessels will simply stay intact, that's ok. Just discard this larger chunks.
Your ground placenta should look like this:
STEP 13:
Pour all the ground placenta into a bowl or onto a deep plate.
STEP 14:
Take the two parts of your capsules (we used organic vegetarian gelatin capsules, sizes 0 and 00. 0 seemed to work best for me and is a little smaller.) and scoop them towards each other in the freshly ground powder, making sure to seal tightly. Place in "resting place" on paper towel.
STEP 15:
Discard any excess capsules that came in contact with the powder as well as any excess powder that you couldn't encapsulate.
STEP 16:
Wipe down the pills to remove any loose powder, grooved paper towels work great. Then place in jar/bottle/bag to give to mama. Store in fridge or freezer.
We were able to yield 122 good size capsules from this placenta. Mom takes about 3 tablets 2-3 times daily for general use or up to 8 a day if using to stave off post partum depression.
A huge thank you to the lovely Jessica J. for teaching Doula Faye and myself this art of placenta encapsulating. I am happy to offer this service to anyone who might be interested and we'd love to spread the knowledge, know-how and fun of this ancient art.
5.10.2010
Placenta Encapsulation-Phase 1
This is honestly not something I would have ever thought I'd think was beneficial or anything short of freaky. However, the more I learn about pregnancy and childbirth, especially the benefits of natural remedies or alternatives, the more this became a topic of interest. I'm sad now that I never got to examine my placenta much less use it to my advantage health wise. Encapsulation is not consumption in the sense that you're "eating" your placenta. It is the process in which you cook and dry it with herbs and put it in pill form to take post partum.
For more information on the benefits of placenta encapsulation and why many women choose this option (or perhaps to learn of the benefits for yourself) please visit: http://placentabenefits.info/about.asp
What you need:
*Dissection kit (surgical scissors, scalpel, tweezers)
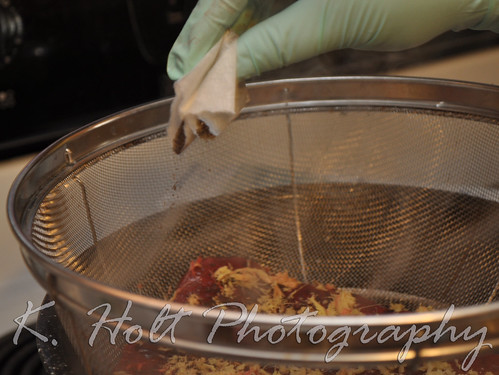
*Sterile Gloves
*Strainer
*Large Pot
*Baking tray
*Oven/dehydrator
You must only use these items for placenta encapsulation. If you're doing this regularly, you need to make sure you have a separate baking tray only for placentas, a separate pot only for placentas, a separate strainer...you get it.
STEP 1:
Wipe placenta clean with gauze or cloth, removing as much blood/debris as possible.

STEP 2:
Remove membrane (sac) with scissors, following the margin of the placenta.

-Puncture hole in membrane with sharp point of scissors and follow along placenta's edge, removing as much as possible. You can try to remove the membrane from the fetal side of the placenta as well.

STEP 3:
Using scissors, remove cord at base.

STEP 4:
Fill pot about 1/2 way with water so that strainer can sit above water level, floating freely without touching the water.
-Grate fresh ginger over placenta, covering lightly.

-Pour ground tea (chai is good, vanilla chai smells heavenly) over placenta, 3-5 bags depending on size.
-squirt with lemon.
STEP 5:
Place placenta in strainer over water, remember water should not touch placenta.

STEP 6:
Once boiling, let steam for 20 minutes, placenta will shrink.


STEP 7:
Remove steamed placenta from strainer and place on non-stick baking tray.

STEP 8:
With scalpel and tweezers, cut into even strips.


STEP 9:
Arrange evenly on tray to allow air flow.

STEP 10:
Place in oven 200-225 degrees and bake for 8-10 hours.

Pieces should be completely dry, black and not at all rubbery.
***Phase 2 tomorrow!***
This process has been not only fun but VERY informational. The placenta is an AMAZING organ. Something that only begins to grow as life begins and continues to grow with your baby, providing nourishment during your pregnancy. How awesome that it's amazing benefits don't end there? I hope you enjoyed what I've shared so far today and look forward to the rest of the process and sharing that with you tomorrow.
Please post any questions or discussion below.
For more information on the benefits of placenta encapsulation and why many women choose this option (or perhaps to learn of the benefits for yourself) please visit: http://placentabenefits.info/about.asp
What you need:
*Dissection kit (surgical scissors, scalpel, tweezers)
*Sterile Gloves
*Strainer
*Large Pot
*Baking tray
*Oven/dehydrator
You must only use these items for placenta encapsulation. If you're doing this regularly, you need to make sure you have a separate baking tray only for placentas, a separate pot only for placentas, a separate strainer...you get it.
STEP 1:
Wipe placenta clean with gauze or cloth, removing as much blood/debris as possible.
STEP 2:
Remove membrane (sac) with scissors, following the margin of the placenta.
-Puncture hole in membrane with sharp point of scissors and follow along placenta's edge, removing as much as possible. You can try to remove the membrane from the fetal side of the placenta as well.
STEP 3:
Using scissors, remove cord at base.
STEP 4:
Fill pot about 1/2 way with water so that strainer can sit above water level, floating freely without touching the water.
-Grate fresh ginger over placenta, covering lightly.
-Pour ground tea (chai is good, vanilla chai smells heavenly) over placenta, 3-5 bags depending on size.
-squirt with lemon.
STEP 5:
Place placenta in strainer over water, remember water should not touch placenta.
STEP 6:
Once boiling, let steam for 20 minutes, placenta will shrink.
STEP 7:
Remove steamed placenta from strainer and place on non-stick baking tray.
STEP 8:
With scalpel and tweezers, cut into even strips.
STEP 9:
Arrange evenly on tray to allow air flow.
STEP 10:
Place in oven 200-225 degrees and bake for 8-10 hours.
Pieces should be completely dry, black and not at all rubbery.
***Phase 2 tomorrow!***
This process has been not only fun but VERY informational. The placenta is an AMAZING organ. Something that only begins to grow as life begins and continues to grow with your baby, providing nourishment during your pregnancy. How awesome that it's amazing benefits don't end there? I hope you enjoyed what I've shared so far today and look forward to the rest of the process and sharing that with you tomorrow.
Please post any questions or discussion below.
Solids: The When, What and HOW.
WHEN?
The AAP states that all infants should be exclusively breastfed for 6 months of life and then at least a year or however long is mutually desired.
Many people don't fully understand what "exclusively" breastfeeding means. It means nothing but breastmilk: no formula, no solids.
Why wait 6 months, why not 4?
A baby's digestive tract matures enough for solid foods (those that aren't breastmilk) between 4 and 6 months of age. Waiting until 6 months ensures your baby's digestive tract can tolerate solid foods. Many of the problems associated with early solids do not show up until later in life and many parents and/or doctors never make the association. It's thanks to many years of studies and the advanced knowledge we've gained about infant's bodies that we know waiting the six month MINIMUM is ideal for optimal health, now and in the future.
Another point often left out of the solid discussion is watching for signs of readiness. Just because your baby is 6 months old doesn't mean they are ready, and just because they've met all the signs of readiness doesn't mean you shouldn't wait until they are 6 months old.
Signs that indicate baby is developmentally ready for solids include:
* Baby can sit up well without support.
* Baby has lost the tongue-thrust reflex and does not automatically push solids out of his mouth with his tongue.
* Baby is ready and willing to chew.
* Baby is developing a “pincer” grasp, where he picks up food or other objects between thumb and forefinger. Using the fingers and scraping the food into the palm of the hand (palmar grasp) does not substitute for pincer grasp development.
* Baby is eager to participate in mealtime and may try to grab food and put it in his mouth.
Baby really needs most/all of these stages to be met as WELL as the 6 month minimum age before they're ready for solids.
A reminder: Solids are *only* for exploration and taste in the first year. They do not replace breastmilk, they are not a nutritional supplement to breastmilk and they should always be given AFTER nursing session. Solids are the first step in weaning.
For more information on solids, visit this great link:
http://www.kellymom.com/nutrition/solids/solids-when.html
What have you learned over the years as to how to approach solids? Did you learn anything knew today? What questions might you ask?
WHAT?
Most parents today think the first introduction to food should be fortified rice cereal. Many pediatricians praise that little box of mush. But, how good IS rice cereal, or any cereal, for your little baby?
More on rice cereal: http://www.homemade-baby-food-recipes.com/best-first-food-for-baby.html
You can SKIP the cereal altogether and go for healthy, fresh foods instead. Remember that some foods are unsafe for infants (eggs, peanut butter and milk. Dairy can be added around 9 months old in the form of yogurt, cheese, etc).
Avocado is a great first food as it's mostly bland and high in natural fats, which are important for a developing infant. Many moms will mix breastmilk with their first solid feedings, but it's not necessary. Read your baby, watch for their cues. Let baby take the wheel, too, with exploring solids and don't be afraid of the mess.
Always wait a few days between new foods to watch for possible allergies/reactions and don't over-feed solids.
HOW?
Like I said, let baby take the wheel. Put some food down in front of him/her, sit next to them and watch him explore and enjoy. If baby has met the required milestones for starting solids, then they should be able to pinch and put to mouth any bits of food. If they are unsure of what to do, offer a little taste to intrigue them.
Take it SLOW.
There is no rush to get your baby to eat food. They are getting all the nutrition they need from your milk, this is just for fun and to help them learn so that by about a year old, they are able to eat more meals.
It's always important to listen to your baby, but you have to maintain a sense of responsibility.
Your baby COULD over eat, so don't let them eat more than an ounce or two.
Always wait at LEAST 6 months and make sure all milestones of solids readiness are met.
Avoid known allergens and always watch for reactions no matter what it is you've fed them.
Always wait a few days between trying new foods.
Don't rush, go at your baby's pace.
Have fun!
5.09.2010
Epidural Epidemic - Drugs in Labor: Are They Really Necessary. . . or Even Safe?
Just had to share this well written, well cited article. I do not hate women for getting epidurals, I hate the cultural fears and over-management of childbirth by Obs and CNMs that has caused them to think they NEED it and led them to LIE on it's safety. Please, take control of your labor and delivery. *Know* the risks of epidurals and other interventions, learn when they ARE necessary and how to avoid them. Look for alternatives to managing pain and labor because they DO exist, they ARE effective and they leave you feeling more positive and accomplished about your birth. It's not a slight against you, it's not an insult to women who've gotten epidurals (I'm ONE of those women!) it's about doing BETTER and becoming more INFORMED for yourself and your baby.
Epidural Epidemic - Drugs in Labor: Are They Really Necessary. . . or Even Safe?
By Joanne Dozer and Shannon Baruth
Issue 95, July/August 1999
The use of epidurals is so common today that many perinatal professionals are calling the 1990s the age of the epidural epidemic. Believed by many in the medical profession to be safe and effective, the epidural seems now to be regarded as a veritable panacea for dealing with the pain of childbirth.
It is true that most women experience pain during the course of labor. This pain can be intense and very real, even for those who have prepared for it. But pain is only one of many possible sensations and experiences that characterize the experience of giving birth. Barbara Katz Rothman, a sociologist who studies birth in America, writes that in the medical management of childbirth, the experience of the mother is viewed by physicians as pain: pain experienced and pain to be avoided.1 Having experienced childbirth ourselves, we have great compassion for women in painful labors. However, we also feel a responsibility to mothers and their babies to explore issues concerning the use of epidural anesthesia in labor issues that are seldom discussed prenatally.
Several factors make the use of epidurals potentially hazardous. The Physician’s Desk Reference cautions that local anesthetics - the type used in epidurals - rapidly cross the placenta. When used for epidural blocks, anesthesia can cause varying degrees of maternal, fetal, and neonatal toxicity which can result in the following side effects: hypotension, urinary retention, fecal and urinary incontinence, paralysis of lower extremities, loss of feeling in the limbs, headache, backache, septic meningitis, slowing of labor, increased need for forceps and vacuum deliveries, cranial nerve palsies, allergic reactions, respiratory depression, nausea, vomiting, and seizures.2 In addition, a piece of the catheter that delivers the drug into the duraregion of the back may break off and be left in the woman, a dangerous risk that necessitates surgical removal. One of the most well-known side effects of spinal anesthesia is a spinal headache. Depending on the amount of anesthetic used and how the catheter was placed, the headache can be mild or severe, lasting between one and ten days after the birth. This is not how any of us wants to feel in our first days and hours with our newborn.
Epidurals also have been linked to an overall increase in operative deliveries: cesareans, forceps deliveries, and vacuum extractions. A meta-analysis of the effects of epidural anesthesia on the rate of cesarean deliveries was undertaken by a group of physicians who examined, categorized, and analyzed all available literature. Eight primary studies revealed that the rate of cesarean section was 10 percentage points higher in the women who had received epidural anesthesia. One study actually found that the cesarean rate increased to 50 percent when the epidural was given at 2 cm dilation, 33 percent at 3 cm, and 26 percent at 4 cm.3 What caused this increase? In the first stage of labor, the muscles of the pelvic floor may become slack from the numbing effects of the epidural, causing the baby to change an otherwise ideal position or fail to descend into the pelvic cavity. In the second stage of labor, the anesthetized woman often is unable to push effectively since she cannot feel her muscles. When the baby does not descend properly or is malpositioned, progress can slow or stop, resulting in a longer labor and the increased possibility of a cesarean section, vacuum extraction, or forceps delivery.
In addition, epidurals usually slow contractions, which prompts medical personnel to administer intravenous Pitocin in order to strengthen them and increase their frequency. Even with Pitocin, which carries its own set of risks, an anesthetized labor may remain prolonged, risking a difficult labor with lack of progress. Prolonged labors put both mother and baby at greater risk of infection, necessitating the use of antibiotics. The longer a labor and slower the progress, the more likely it will end in a forceps, vacuum, or cesarean delivery. Since cesarean section is a major surgery, it strongly influences a woman’s recovery and the initiation of breastfeeding. Of course, the rate of postpartum infection is much higher with cesarean births. All vacuum extraction and forceps deliveries increase the risk of morbidity and birth injuries.
Another effect of epidurals during labor is the creation of hypotension in the mother, which can lead to bradycardia (a decrease in the heart rate) in the fetus. All types of anesthesia, including epidurals, can negatively affect the baby’s heart rate, possibly leading to fetal distress and necessitating an operative delivery. The newborn can continue to have breathing difficulties after birth, requiring supplemental oxygen or even resuscitation. While these problems may be resolved immediately following the birth, they often require the mother to be separated from her baby for neonatal nursery observation. This separation delays bonding and initial feeding. In addition, poor muscle tone and increased acidity in the baby’s blood due to bradycardia and oxygen deprivation may affect her ability to suck effectively, hampering initial attempts at early breastfeeding.
A mother’s temperature may become elevated with the use of epidural anesthesia, resulting in the infant being taken to the nursery and given a full work-up for possible infection. This may include extensive blood work and a spinal tap.4, 5
Furthermore, though epidurals usually remove all sensation in the lower body, "windows" can occur which leave the woman experiencing the intensity of her labor (perhaps on one side of her body) but with extremely limited mobility - obviously hindering her ability to cope with her contractions.6 The idea that pain medication can play a role in "natural childbirth" is deceptive, despite the assurance of the authors of What to Expect When You’re Expecting that "...wanting relief from excruciating pain is natural...therefore pain relief medication can play a role in natural childbirth."7 This is rather twisted logic, since the concept of natural childbirth depends on the mother experiencing both mental and physical sensations of labor. The epidural may allow a woman to be awake and aware of what is happening, but she will not be experiencing a natural labor as she will be numb to any physical sensations below the waist. A split between the mind and the body is effectively created with this anesthetic, disengaging her mind from her physical feelings. Could such disconnection be natural childbirth? Robbie Davis-Floyd, an anthropologist who studies birth in America, argues that the woman in labor with an epidural "...is separated as a person as effectively as she can be from the part of her that is giving birth."8 There is an eerie quality to this kind of birth; the mother is robbed of her own connection to her power and life-creative force. She loses the opportunity to experience the inherent wisdom of the body and its ability to birth without interference. Indeed, most women who have felt childbirth agree that it was a deep, enriching, and positive experience.
What alternatives do women have for the relief of pain in labor? Unfortunately, many women enter the birth experience with a strong belief that birth is something horrible and nightmarish. They are already filled with fear, not only for their own and their baby’s safety but also about what they have heard is the unbearable pain of childbirth. Another important fear is that of "losing control" during labor and delivery. A mother often is labeled out of control if she expresses the natural, primal sounds of labor. Technologically oriented medical practitioners who are sure that childbirth is something to be wrestled into submission feel that the sound of a mother wailing in pain is a sign that she is "losing it" and ought to be medicated. In hospitals, mothers are often told by well-meaning nurses to be quiet so as not to disturb the other "patients." But release of sound is a natural way to express and release painful - and intense - sensations. Suppressing a mother’s natural instincts to move around freely and make noise in labor will increase her actual pain. The prepared childbirth movement - in particular the Lamaze technique - has been successful for some women by helping them remain "in control" by training for structured labor breathing. However, some women actually do connect to their body rhythms and natural breathing patterns in labor, and if they are more loyal to themselves than to their training, they may be seen as wild, out-of-control "Lamaze failures." This failure is defined as their inability in labor to be mannerly and controlled. In fact, one of the primary psychological reasons for lack of progress and cesareans is a fearful mother’s unconscious attempts to control the intensity of her labor. Her lack of progress is due to her inability to let go and surrender. Mothers are told they must be in control when actually they need to let go.
So how does a mother let go and find her way through the pain of labor? First, she needs to give birth where she feels safe. For some women this may mean a medicalized hospital birth; others may feel safest at home or in an alternative birthing center. Most women find that they feel safest in the loving hands of a practitioner with whom they have developed a supportive and loving relationship. This person may be a special kind of doctor or it may be a midwife. Midwives specialize in personalized, supportive perinatal care. Support is the best form and prime source of non-pharmacological pain relief. Support can also come from the love and care of a partner. If you are having your baby in a hospital, it may be worthwhile to secure the help of a knowledgeable friend or a doula. Support can be active: massage, breathing together, encouraging words and attentiveness, and reassurance that what it happening is normal and that you are handling it well. Other support can be more passive: a midwife’s calm demeanor, a gentle nurse’s presence, the peaceful attentions of loved ones. A laboring mother needs to feel safe, loved, and accepted. And when she is, whether she screams, hollers, whines, moans, bargains, begs, or just plain doesn’t act "civilized," giving birth vaginally without medication is a triumph in itself.
One of the ways to endure labor is to recognize (ideally, during one’s prenatal education) the connection between fear, tension, and pain - the "fear-tension-pain syndrome." Basically, when a mother feels fear, she will be tense and experience more pain. Relaxation relieves the tension that helps create the sensation of intense pain. The notion of a relaxing labor might seem crazy, but it is possible, and we have seen it many times. Of course, a mother will feel more relaxed and safer in the birth environment of her choice and with her chosen caregivers. Perhaps the more the mother chooses about her birth environment, the more fully she can relax.
Childbirth education classes that focus on birth as natural and normal encourage women to trust the birthing process. Birthing is full of new sensations which can be frightening and difficult to integrate; some women tell us that they felt they might split in two! Understanding the reasons behind the sensations can make them more manageable, since we fear most that which we do not understand. Another key concept in prenatal education is truly believing we can birth our babies, just as women have done for ages. The world was well-populated long before modern obstetrics, and today the lowest maternal and infant mortality and morbidity rates are in the countries where natural, midwife-assisted births are the norm.
Not only can we birth our babies naturally, we can birth in our own style. Birth doesn’t need to be performed in any specific way. It is a woman’s right to create her labor her way, and she needs to be accepted for her way of doing it. She may find help in deep breathing, light breathing, dancing, singing, yelling, screaming, moaning, crying, walking, or bathing. She needs support for whatever works to assist her to birth her baby. Soaking in water can also help tremendously in reducing pain in labor. Prenatal yoga can be extremely helpful since it teaches women to relax by using deep breathing techniques and imagery. Both of these methods help her to connect more profoundly to her body and baby.
No woman should feel like a failure for having used pain relief medication during labor. There is a time and place for it in specific circumstances, and epidurals may be very effective. However, the decision to use an epidural should be an educated one, made only after all other options have been exhausted. Birthing is hard work. It is sweaty, noisy, and emotional, and it always requires our full attention. If we accept this, and stop trying to make birthing "civilized," we can help mothers to endure and cope.
Assisting a woman who is giving birth also is hard work, requiring education, love, and our full attention. Supporting birthing women in this way results in less fear, less pain, and a decrease in the need and desire for epidural anesthesia. The satisfaction of a natural birth - including the sheer endurance of pain and sometimes overwhelming sensations - is accompanied by great joy, even ecstasy. The realization of all these complex emotions is experienced not only by the mother but also by her partner and those who assist, attend, and support her in labor. The sense of joy and accomplishment from a natural birth is the right of every woman - and a wonderful gift to any newborn in those very special, first moments of life. NOTES
1. Barbara Katz Rothman, In Labor: Women and Power in the Birthplace, (New York: W.W. Norton & Company, 1991), 80
2. Sifton, David W. Ed., The Physician’s Desk Reference (Montvale, NJ: Medical Economics Company, 1996), 2318.
3. Joseph Gambone, D.O., and Katherine Kahn, M.D., "The Effect of Epidural Analgesia for Labor on the Cesarean Delivery Rate," Obstetrics and Gynecology 83, No. 6 (June 1994):1045-1052; Thorp, M.D., et. al., "Epidural Anesthesia and Cesarean Section for Dystocia: Risk Factors in Multiparas," American Journal of Perinatology 8, No. 6: 402-410; Thorp, M.D., et. al., "The Effect of Intrapartum Epidural Analgesia on Nulliparous Labor: A Randomized, Controlled, Prospective Trial," American Journal of Obstetrics and Gynecology 169, No. 4: 851-858.
4. Author’s name, "The Bad News About Epidurals," Time, March 24, 1997, page 40.
5. Fusi, et al., "Maternal Pyrexia Associated with the Use of Epidural Analgesia in Labour," Lancet 8649 (3 June 1989): 1250.
6. B.M. Morgan, S. Rehor, and P.J. Lewis, "Epidural Anesthesia for Uneventful Labor," Anesthesia 35 (1980): 57-60.
7. Arlene Eisenberg, Heidi Murkhoff, and Sandee Hathaway, What to Expect When You’re Expecting (New York: Workman Publishing, 1984), 227.
8 Robbie E. Davis-Floyd, Birth as an American Rite of Passage (Los Angeles: University of California Press, 1992), 115. OTHER REFERENCES
Griffin, Nancy. "The Epidural Express: Real Reasons Not to Jump On Board," Mothering , Spring, 1997.
Mitford, Jessica. The American Way of Birth. Dutton, New York, 1992.
Morton, Sally, Ph.D.; Williams, Mark, M.D.; Keller, Emmett, PhD.; Peaceman, M.D., et. al., "Factors that influence route of delivery - active vs. traditional labor management," American Journal of Obstetrics and Gynecology, Vol. 169, No. 4, 940-944.
Sepkowski, Lester, Ostheimer and Brazelton. "The effects of maternal epidural anesthesia on neonatal behavior during the first month," Development of Medicine and Child Neurology, 1992, 34, 1072-1080. This article was originally edited by Leslie Hauslein. Shannon Baruth is a birth assistant, apprenticing midwife, mother to Cassidy Rose (2 1/2) and Sage (14 months), and partner to Michael. She graduated from Bryn Mawr College in 1997 with a bachelor’s degree in anthropology. She resides in rural Wisconsin. Joann Dozer is a registered nurse and CPM who has been delivering babies at home for more than 20 years. A trained Gestalt therapist, she provides counseling and workshops for women and couples. Joanne is the mother of Scott, born in 1968 in a hospital delivery that included the use of Demerol and spinal anesthesia; Lianna, born in 1973 in the birthing room of an Amish midwife’s home; and Emily, born in 1976 at home with a midwife and doctor.
Epidural Epidemic - Drugs in Labor: Are They Really Necessary. . . or Even Safe?
By Joanne Dozer and Shannon Baruth
Issue 95, July/August 1999
The use of epidurals is so common today that many perinatal professionals are calling the 1990s the age of the epidural epidemic. Believed by many in the medical profession to be safe and effective, the epidural seems now to be regarded as a veritable panacea for dealing with the pain of childbirth.
It is true that most women experience pain during the course of labor. This pain can be intense and very real, even for those who have prepared for it. But pain is only one of many possible sensations and experiences that characterize the experience of giving birth. Barbara Katz Rothman, a sociologist who studies birth in America, writes that in the medical management of childbirth, the experience of the mother is viewed by physicians as pain: pain experienced and pain to be avoided.1 Having experienced childbirth ourselves, we have great compassion for women in painful labors. However, we also feel a responsibility to mothers and their babies to explore issues concerning the use of epidural anesthesia in labor issues that are seldom discussed prenatally.
Several factors make the use of epidurals potentially hazardous. The Physician’s Desk Reference cautions that local anesthetics - the type used in epidurals - rapidly cross the placenta. When used for epidural blocks, anesthesia can cause varying degrees of maternal, fetal, and neonatal toxicity which can result in the following side effects: hypotension, urinary retention, fecal and urinary incontinence, paralysis of lower extremities, loss of feeling in the limbs, headache, backache, septic meningitis, slowing of labor, increased need for forceps and vacuum deliveries, cranial nerve palsies, allergic reactions, respiratory depression, nausea, vomiting, and seizures.2 In addition, a piece of the catheter that delivers the drug into the duraregion of the back may break off and be left in the woman, a dangerous risk that necessitates surgical removal. One of the most well-known side effects of spinal anesthesia is a spinal headache. Depending on the amount of anesthetic used and how the catheter was placed, the headache can be mild or severe, lasting between one and ten days after the birth. This is not how any of us wants to feel in our first days and hours with our newborn.
Epidurals also have been linked to an overall increase in operative deliveries: cesareans, forceps deliveries, and vacuum extractions. A meta-analysis of the effects of epidural anesthesia on the rate of cesarean deliveries was undertaken by a group of physicians who examined, categorized, and analyzed all available literature. Eight primary studies revealed that the rate of cesarean section was 10 percentage points higher in the women who had received epidural anesthesia. One study actually found that the cesarean rate increased to 50 percent when the epidural was given at 2 cm dilation, 33 percent at 3 cm, and 26 percent at 4 cm.3 What caused this increase? In the first stage of labor, the muscles of the pelvic floor may become slack from the numbing effects of the epidural, causing the baby to change an otherwise ideal position or fail to descend into the pelvic cavity. In the second stage of labor, the anesthetized woman often is unable to push effectively since she cannot feel her muscles. When the baby does not descend properly or is malpositioned, progress can slow or stop, resulting in a longer labor and the increased possibility of a cesarean section, vacuum extraction, or forceps delivery.
In addition, epidurals usually slow contractions, which prompts medical personnel to administer intravenous Pitocin in order to strengthen them and increase their frequency. Even with Pitocin, which carries its own set of risks, an anesthetized labor may remain prolonged, risking a difficult labor with lack of progress. Prolonged labors put both mother and baby at greater risk of infection, necessitating the use of antibiotics. The longer a labor and slower the progress, the more likely it will end in a forceps, vacuum, or cesarean delivery. Since cesarean section is a major surgery, it strongly influences a woman’s recovery and the initiation of breastfeeding. Of course, the rate of postpartum infection is much higher with cesarean births. All vacuum extraction and forceps deliveries increase the risk of morbidity and birth injuries.
Another effect of epidurals during labor is the creation of hypotension in the mother, which can lead to bradycardia (a decrease in the heart rate) in the fetus. All types of anesthesia, including epidurals, can negatively affect the baby’s heart rate, possibly leading to fetal distress and necessitating an operative delivery. The newborn can continue to have breathing difficulties after birth, requiring supplemental oxygen or even resuscitation. While these problems may be resolved immediately following the birth, they often require the mother to be separated from her baby for neonatal nursery observation. This separation delays bonding and initial feeding. In addition, poor muscle tone and increased acidity in the baby’s blood due to bradycardia and oxygen deprivation may affect her ability to suck effectively, hampering initial attempts at early breastfeeding.
A mother’s temperature may become elevated with the use of epidural anesthesia, resulting in the infant being taken to the nursery and given a full work-up for possible infection. This may include extensive blood work and a spinal tap.4, 5
Furthermore, though epidurals usually remove all sensation in the lower body, "windows" can occur which leave the woman experiencing the intensity of her labor (perhaps on one side of her body) but with extremely limited mobility - obviously hindering her ability to cope with her contractions.6 The idea that pain medication can play a role in "natural childbirth" is deceptive, despite the assurance of the authors of What to Expect When You’re Expecting that "...wanting relief from excruciating pain is natural...therefore pain relief medication can play a role in natural childbirth."7 This is rather twisted logic, since the concept of natural childbirth depends on the mother experiencing both mental and physical sensations of labor. The epidural may allow a woman to be awake and aware of what is happening, but she will not be experiencing a natural labor as she will be numb to any physical sensations below the waist. A split between the mind and the body is effectively created with this anesthetic, disengaging her mind from her physical feelings. Could such disconnection be natural childbirth? Robbie Davis-Floyd, an anthropologist who studies birth in America, argues that the woman in labor with an epidural "...is separated as a person as effectively as she can be from the part of her that is giving birth."8 There is an eerie quality to this kind of birth; the mother is robbed of her own connection to her power and life-creative force. She loses the opportunity to experience the inherent wisdom of the body and its ability to birth without interference. Indeed, most women who have felt childbirth agree that it was a deep, enriching, and positive experience.
What alternatives do women have for the relief of pain in labor? Unfortunately, many women enter the birth experience with a strong belief that birth is something horrible and nightmarish. They are already filled with fear, not only for their own and their baby’s safety but also about what they have heard is the unbearable pain of childbirth. Another important fear is that of "losing control" during labor and delivery. A mother often is labeled out of control if she expresses the natural, primal sounds of labor. Technologically oriented medical practitioners who are sure that childbirth is something to be wrestled into submission feel that the sound of a mother wailing in pain is a sign that she is "losing it" and ought to be medicated. In hospitals, mothers are often told by well-meaning nurses to be quiet so as not to disturb the other "patients." But release of sound is a natural way to express and release painful - and intense - sensations. Suppressing a mother’s natural instincts to move around freely and make noise in labor will increase her actual pain. The prepared childbirth movement - in particular the Lamaze technique - has been successful for some women by helping them remain "in control" by training for structured labor breathing. However, some women actually do connect to their body rhythms and natural breathing patterns in labor, and if they are more loyal to themselves than to their training, they may be seen as wild, out-of-control "Lamaze failures." This failure is defined as their inability in labor to be mannerly and controlled. In fact, one of the primary psychological reasons for lack of progress and cesareans is a fearful mother’s unconscious attempts to control the intensity of her labor. Her lack of progress is due to her inability to let go and surrender. Mothers are told they must be in control when actually they need to let go.
So how does a mother let go and find her way through the pain of labor? First, she needs to give birth where she feels safe. For some women this may mean a medicalized hospital birth; others may feel safest at home or in an alternative birthing center. Most women find that they feel safest in the loving hands of a practitioner with whom they have developed a supportive and loving relationship. This person may be a special kind of doctor or it may be a midwife. Midwives specialize in personalized, supportive perinatal care. Support is the best form and prime source of non-pharmacological pain relief. Support can also come from the love and care of a partner. If you are having your baby in a hospital, it may be worthwhile to secure the help of a knowledgeable friend or a doula. Support can be active: massage, breathing together, encouraging words and attentiveness, and reassurance that what it happening is normal and that you are handling it well. Other support can be more passive: a midwife’s calm demeanor, a gentle nurse’s presence, the peaceful attentions of loved ones. A laboring mother needs to feel safe, loved, and accepted. And when she is, whether she screams, hollers, whines, moans, bargains, begs, or just plain doesn’t act "civilized," giving birth vaginally without medication is a triumph in itself.
One of the ways to endure labor is to recognize (ideally, during one’s prenatal education) the connection between fear, tension, and pain - the "fear-tension-pain syndrome." Basically, when a mother feels fear, she will be tense and experience more pain. Relaxation relieves the tension that helps create the sensation of intense pain. The notion of a relaxing labor might seem crazy, but it is possible, and we have seen it many times. Of course, a mother will feel more relaxed and safer in the birth environment of her choice and with her chosen caregivers. Perhaps the more the mother chooses about her birth environment, the more fully she can relax.
Childbirth education classes that focus on birth as natural and normal encourage women to trust the birthing process. Birthing is full of new sensations which can be frightening and difficult to integrate; some women tell us that they felt they might split in two! Understanding the reasons behind the sensations can make them more manageable, since we fear most that which we do not understand. Another key concept in prenatal education is truly believing we can birth our babies, just as women have done for ages. The world was well-populated long before modern obstetrics, and today the lowest maternal and infant mortality and morbidity rates are in the countries where natural, midwife-assisted births are the norm.
Not only can we birth our babies naturally, we can birth in our own style. Birth doesn’t need to be performed in any specific way. It is a woman’s right to create her labor her way, and she needs to be accepted for her way of doing it. She may find help in deep breathing, light breathing, dancing, singing, yelling, screaming, moaning, crying, walking, or bathing. She needs support for whatever works to assist her to birth her baby. Soaking in water can also help tremendously in reducing pain in labor. Prenatal yoga can be extremely helpful since it teaches women to relax by using deep breathing techniques and imagery. Both of these methods help her to connect more profoundly to her body and baby.
No woman should feel like a failure for having used pain relief medication during labor. There is a time and place for it in specific circumstances, and epidurals may be very effective. However, the decision to use an epidural should be an educated one, made only after all other options have been exhausted. Birthing is hard work. It is sweaty, noisy, and emotional, and it always requires our full attention. If we accept this, and stop trying to make birthing "civilized," we can help mothers to endure and cope.
Assisting a woman who is giving birth also is hard work, requiring education, love, and our full attention. Supporting birthing women in this way results in less fear, less pain, and a decrease in the need and desire for epidural anesthesia. The satisfaction of a natural birth - including the sheer endurance of pain and sometimes overwhelming sensations - is accompanied by great joy, even ecstasy. The realization of all these complex emotions is experienced not only by the mother but also by her partner and those who assist, attend, and support her in labor. The sense of joy and accomplishment from a natural birth is the right of every woman - and a wonderful gift to any newborn in those very special, first moments of life. NOTES
1. Barbara Katz Rothman, In Labor: Women and Power in the Birthplace, (New York: W.W. Norton & Company, 1991), 80
2. Sifton, David W. Ed., The Physician’s Desk Reference (Montvale, NJ: Medical Economics Company, 1996), 2318.
3. Joseph Gambone, D.O., and Katherine Kahn, M.D., "The Effect of Epidural Analgesia for Labor on the Cesarean Delivery Rate," Obstetrics and Gynecology 83, No. 6 (June 1994):1045-1052; Thorp, M.D., et. al., "Epidural Anesthesia and Cesarean Section for Dystocia: Risk Factors in Multiparas," American Journal of Perinatology 8, No. 6: 402-410; Thorp, M.D., et. al., "The Effect of Intrapartum Epidural Analgesia on Nulliparous Labor: A Randomized, Controlled, Prospective Trial," American Journal of Obstetrics and Gynecology 169, No. 4: 851-858.
4. Author’s name, "The Bad News About Epidurals," Time, March 24, 1997, page 40.
5. Fusi, et al., "Maternal Pyrexia Associated with the Use of Epidural Analgesia in Labour," Lancet 8649 (3 June 1989): 1250.
6. B.M. Morgan, S. Rehor, and P.J. Lewis, "Epidural Anesthesia for Uneventful Labor," Anesthesia 35 (1980): 57-60.
7. Arlene Eisenberg, Heidi Murkhoff, and Sandee Hathaway, What to Expect When You’re Expecting (New York: Workman Publishing, 1984), 227.
8 Robbie E. Davis-Floyd, Birth as an American Rite of Passage (Los Angeles: University of California Press, 1992), 115. OTHER REFERENCES
Griffin, Nancy. "The Epidural Express: Real Reasons Not to Jump On Board," Mothering , Spring, 1997.
Mitford, Jessica. The American Way of Birth. Dutton, New York, 1992.
Morton, Sally, Ph.D.; Williams, Mark, M.D.; Keller, Emmett, PhD.; Peaceman, M.D., et. al., "Factors that influence route of delivery - active vs. traditional labor management," American Journal of Obstetrics and Gynecology, Vol. 169, No. 4, 940-944.
Sepkowski, Lester, Ostheimer and Brazelton. "The effects of maternal epidural anesthesia on neonatal behavior during the first month," Development of Medicine and Child Neurology, 1992, 34, 1072-1080. This article was originally edited by Leslie Hauslein. Shannon Baruth is a birth assistant, apprenticing midwife, mother to Cassidy Rose (2 1/2) and Sage (14 months), and partner to Michael. She graduated from Bryn Mawr College in 1997 with a bachelor’s degree in anthropology. She resides in rural Wisconsin. Joann Dozer is a registered nurse and CPM who has been delivering babies at home for more than 20 years. A trained Gestalt therapist, she provides counseling and workshops for women and couples. Joanne is the mother of Scott, born in 1968 in a hospital delivery that included the use of Demerol and spinal anesthesia; Lianna, born in 1973 in the birthing room of an Amish midwife’s home; and Emily, born in 1976 at home with a midwife and doctor.
5.07.2010
Breastfeeding Joys
I thought today I'd share a great blog written by a friend, activist and doula. She writes on the joys of breastfeeding.
Visit her blog. She's new to this but I think you'll enjoy what she'll have to say. She is filled with warmth, knowledge and compassion.

Being a Mom of two under two can be very challenging at times. From changing diapers to cleaning banana out of the carpet, all while trying to get dinner on the table by 5 and keep up on the Laundry. There is little time to stop and take time for your self.
There seems to be only brief moments when the world comes to a halt and nothing else seems to matter. It happens a few times throughout the day as you are cleaning, cooking, or chasing your toddler. It even sometimes happens while you are running your errands. You hear a coo, or a fuss and nothing else in the world matters everything stops and its just you and your baby.
Her sweet little lips rooting for the warmth and comfort of the breast, pure satisfaction comes across her little face as she latches on. Her eyes meet yours and your heart swells with love. There is nothing more rewarding.
I have found from the first moment I held my children in my arms I knew I had to provide what was best for them. There is nothing more pure more wonderful and more loving than Breastfeeding your baby. Knowing that my body is capable of fulfilling all the needs of my infant is truly satisfying.
Visit her blog. She's new to this but I think you'll enjoy what she'll have to say. She is filled with warmth, knowledge and compassion.
Joys of Nursing

Being a Mom of two under two can be very challenging at times. From changing diapers to cleaning banana out of the carpet, all while trying to get dinner on the table by 5 and keep up on the Laundry. There is little time to stop and take time for your self.
There seems to be only brief moments when the world comes to a halt and nothing else seems to matter. It happens a few times throughout the day as you are cleaning, cooking, or chasing your toddler. It even sometimes happens while you are running your errands. You hear a coo, or a fuss and nothing else in the world matters everything stops and its just you and your baby.
Her sweet little lips rooting for the warmth and comfort of the breast, pure satisfaction comes across her little face as she latches on. Her eyes meet yours and your heart swells with love. There is nothing more rewarding.
I have found from the first moment I held my children in my arms I knew I had to provide what was best for them. There is nothing more pure more wonderful and more loving than Breastfeeding your baby. Knowing that my body is capable of fulfilling all the needs of my infant is truly satisfying.
5.03.2010
Kids Things Say
Yes, you read that right. The title is fitting, since many times, our toddlers try so hard to imitate what they've heard from us and use it in context, but usually miss one or two things in the process.
Alexander is at that fun stage where his vocabulary is taking off but it his thought process hasn't quite caught up. His new favorite phrase is "Told you! Haha" but he uses it at the most random and inappropriate times. Of course, this just makes it funny and adorable.
What are some cute and crazy things your kids are saying (or have said)?
I love to hear all the funny (or embarrassing) stories!
Alexander is at that fun stage where his vocabulary is taking off but it his thought process hasn't quite caught up. His new favorite phrase is "Told you! Haha" but he uses it at the most random and inappropriate times. Of course, this just makes it funny and adorable.
What are some cute and crazy things your kids are saying (or have said)?
I love to hear all the funny (or embarrassing) stories!
4.04.2010
Natural Mama Meetup
A mutual natural mama and I met the other day for coffee and decided we NEED an anti-mainstream mommy group. Sadly, breastfeeding, cloth diapering, and other things that were once normal are no longer viewed that way. The minority of mothers today who practice these are often outcast, or even mocked, for believing in a better, healthier, natural alternative to disposable products and man-made foods. As a result, it can be difficult to enjoy playgroups when you have nothing in common on the parenting spectrum with the other mothers.
There isn't a huge amount of women in this area who parent this way, but I know there are enough to form a nice group. It will be great for moms to be able to ask for advice on this topics from moms that actually know and can share, rather than from women who will snort and laugh when you talk about your cloth diapers.
If you're in the Turlock, or any of the surrounding area, come by our Facebook page and listen for updates. We look forward to getting this off the ground.
There isn't a huge amount of women in this area who parent this way, but I know there are enough to form a nice group. It will be great for moms to be able to ask for advice on this topics from moms that actually know and can share, rather than from women who will snort and laugh when you talk about your cloth diapers.
If you're in the Turlock, or any of the surrounding area, come by our Facebook page and listen for updates. We look forward to getting this off the ground.
3.01.2010
Who Profits??
**Cross Posted from my other blog**
I'm sharing this article on THIS blog not to argue in favor of homebirth or say that choosing hospital birth is wrong. Like *most* things I post, it's purpose is to educate, share and make you think. Leave your constructive comments below.Who Profits?
Anyone can admit that we are easily influenced and swayed by what seems to be a popular opinion. Most people would agree that it is much easier to be a PART of the masses than to be APART from them.
"What is popular is not always right,
and what is right is not always popular."
When it comes to parenting (specifically birthing and infant care) we are led to believe that our instincts are no longer necessary and that technology knows better than nature. But who profits from this philosophy? Certainly not mother and baby. Instead, there is a very large LITERAL profit to be made off of influencing you in your choices.
There is money to be made off of where you birth, how you birth and also, how you feed and treat your infant. The hospital makes a very large portion of their profit from the labor and delivery ward and let's face it, hospitals are businesses. They do NOT want to lose that money, even if it might mean safer outcomes can occur at home for low risk women. Obstetricians make thousands of dollars off your birth (and prenatal care) whereas homebirth midwives make around $4000 (for both the birth and prenatal care total). A cesarean can cost you more than $20,000 and only costs your OB 30 minutes of work (and a nice early bed time if you aren't "progressing" fast enough). Vaccinations, routine exams and procedures (episiotomy, circumcision, forcep delivery) all take just a moment to do/perform and net a nice profit.
Now, before you stop reading and get angry and tell me I hate OBs and that I think hospitals are evil, let me say, no. OBs are SPECIALISTS. They are INCREDIBLY skilled in saving what needs to be saved BUT for that, I think *most* of them have a difficult time knowing and trusting that birth is normal. If your focus of study is all that can go wrong with something, it's hard NOT to want to act in a precautionary manner. For this, I believe that most OBs truly have women's best interest at heart with certain things. However, there are a few scenarios that are indisputably self centered and dangerous, serving the woman absolutely no benefit.
To continue, it is ignorant to think that every ad or persuasion doesn't have an underlying hidden meaning. Formula companies for example want to make money. They do not care about you and your baby, they care only for the profit. At the beginning, when infant formulas were first introduced, they provided a way for the women who could truly not breastfeed or have a wet nurse a way to provide for their infant children. Again, just like the hospitals, this can be and was life saving for those infants. However, there was profit to be made, a feminist movement of choice and a desire to no longer have to feel tied down to your children...and they marketed that. Today they advertise with such sayings as "Just as good as breastmilk" or "Has all your baby needs!" Stop. Think. Who profits from promoting breastfeeding? The mother and child who nurse. Who profits from promoting formula feeding? The industry.
Am I going to lose sleep over another parents' choices? Nope. But as a parent who did things this way and that way before stepping back and evaluating the choices, I wish only to share the other side of the glass with you. I would never tell a woman what choice she should make, I can only share what I know and what I continue to learn, because I care.
To say that homebirthers are selfish or that it's dangerous, because that is what those who profit from your hospital birth tell you, well...that makes you sound not only uneducated, but silly.
Remember who profits from routine interventions in normal birth: it's not you...and it's certainly not the baby.
2.24.2010
A Day (or 4) in the life...
As a hobby and part time side job, I have a small freelance photography business offering portraits to locals. I've always wanted to participate in a 365 project, where you take a photograph every day for a year. I started "late" rather than on the first day of 2010 and didn't set my goals high. I'm not tracking something or striving for artistry but simply making sure I use my camera EVERY day, regardless of what I end up shooting.
I have a feeling the constant will develop as a catalog of days spent with my babies. So far, on day 4, here are the results:




I have a feeling the constant will develop as a catalog of days spent with my babies. So far, on day 4, here are the results:
I'm glad I finally decided to take on the "challenge". Whether or not great art comes of it, or I simply capture the beauty in every day life I am excited to see where it all goes and to use my camera EVERY single day.
Have you ever done this yourself? (Share a link!)
Want to start one? (Go ahead!)
Have you ever done this yourself? (Share a link!)
Want to start one? (Go ahead!)
2.18.2010
The Co-sleeping Conspiracy
 While pregnant with my first baby, I didn't think much of babies "needing" to sleep anywhere. Yes, we bought a crib and yes, the intention was to have her sleep in it, but I never thought of it as something she HAD to do. It was natural for us, from the very beginning, to snuggle in my bed. After she'd fallen asleep I'd sometimes lay her in her crib, only to bring her in bed with me at the first night time waking. This was just easier, for both of us. Less waking up for her and more z's for mom. Eventually, she naturally slept alone in her crib/bed without needing to come in to mine.
While pregnant with my first baby, I didn't think much of babies "needing" to sleep anywhere. Yes, we bought a crib and yes, the intention was to have her sleep in it, but I never thought of it as something she HAD to do. It was natural for us, from the very beginning, to snuggle in my bed. After she'd fallen asleep I'd sometimes lay her in her crib, only to bring her in bed with me at the first night time waking. This was just easier, for both of us. Less waking up for her and more z's for mom. Eventually, she naturally slept alone in her crib/bed without needing to come in to mine.The same happened with baby number 2. I just gave birth to this precious little thing, that last thing on my mind was being separated from her! I wasn't breastfeeding, but that didn't matter. I was able to snuggle close to her, watch her breathing, comfort her while a bottle was made and keep her warm. Again, she naturally "weaned" from co-sleeping to sleeping in her crib. Both of the girls never had a problem napping in their cribs or even sleeping the first portion of the night there.
While pregnant with my son, my third baby, I began to see a lot of debate show up on co-sleeping. Either I never really paid attention to or noticed it before but apparently, it was a huge controversy. There are even campaigns that slander co-sleepers and parents are almost always blamed in co-sleeping deaths, while crib deaths are referred to as "SIDS". I was pretty shocked, to be honest. I had never researched co-sleeping (during my first two pregnancies I didn't research anything at all!) but I just knew there was nothing dangerous about it. I didn't consume alcohol and then sleep with my babies. I always was careful with pillows and blankets. The once heavy sleeper I was in my high school years disappeared as soon as I became a mom and I was aware of every move my babies made in bed. I didn't see the big deal.
For new parents, there can be a lot of information to take in. We constantly get well meaning, but sometimes awful, advice from family and friends. Many people gasp if you mention you sleep with your baby and they are quick to tell you about all the dangers.
But here's the thing: there are always SAFE and UNSAFE ways to do things, especially co-sleeping.
NEVER:
*Drink alcohol or use drugs and then co-sleep with your baby/child.
*Take medications that make you drowsy (this includes types of cough syrup, tylenol pms, sleeping aids, benadryl, etc)
*Use an excess of pillows and/or blankets.
*Pull the blankets up too far or over baby's head.
*Place your newborn between the wall and you.
ALWAYS:
*keep baby off pillows (mostly for newborns)
*Avoid overly stuffed blankets
*Be aware of where baby is at (when you stir or wake up, check on baby, just as you would in their crib).
For those of you about to become parents, do not worry about what people will think. It IS ok to take your baby to bed with you. Practice common sense safe sleeping, in cribs AND your own bed, and do not be ashamed to say you co-sleep with your little one. Motherhood is tiring and those first few weeks and months are not only an adjustment period but a learning experience. You may swear you'll never co-sleep only to find out it's the only way TO sleep. As with anything else, make sure you have ALL the info. Babies sometimes inexplicably pass away and yes, some babies are killed due to UNSAFE co-sleeping. If you do it, do it safely.
Happy sleeping!
2.11.2010
What's in Breastmilk?
What's in Breast Milk?

The American Academy of Pediatrics (AAP) strongly recommends exclusive breastfeeding for the first six months of life. It is optimal for both babies and mothers. For babies it can protect against infections and reduce the rates of later health problems including diabetes, obesity, and asthma.
For mothers breastfeeding helps the uterus to contract and bleeding to cease more quickly after delivery. Breastfeeding can reduce the risk of breast and ovarian cancer and also provides a great way for mothers to bond with their babies.
Find a Lactation Conultant in Your Area
The advantages of breastfeeding are numerous. Breast milk is ultimately the best source of nutrition for a new baby. Many components in breast milk help protect your baby against infection and disease. The proteins in breast milk are more easily digested than in formula or cow’s milk. The calcium and iron in breast milk are also more easily absorbed.
The following is a brief overview of the components of breast milk and the nutrients they provide for your baby.
Proteins
Human milk contains two types of proteins: whey and casein. Approximately 60% is whey, while 40% is casein. This balance of the proteins allows for quick and easy digestion. If artificial milk, also called formula, has a greater percentage of casein, it will be more difficult for the baby to digest. Approximately 60-80% of all protein in human milk is whey protein. These proteins have great infection-protection properties.
Listed below are specific proteins that are found in breast milk and their benefits:
- Lactoferrin inhibits the growth of iron-dependent bacteria in the gastrointestinal tract. This inhibits certain organisms, such as coliforms and yeast, that require iron.
- Secretory IgA also works to protect the infant from viruses and bacteria, specifically those that the baby, mom, and family are exposed to. It also helps to protect against E. Coli and possibly allergies. Other immunoglobulins, including IgG and IgM, in breast milk also help protect against bacterial and viral infections. Eating fish can help increase the amount of these proteins in your breast milk.
- Lysozyme is an enzyme that protects the infant against E. Coli and Salmonella. It also promotes the growth of healthy intestinal flora and has anti-inflammatory functions.
- Bifidus factor supports the growth of lactobacillus. Lactobacillus is a beneficial bacteria that protects the baby against harmful bacteria by creating an acidic environment where it cannot survive
Fats
Human milk also contains fats that are essential for the health of your baby. It is necessary for brain development, absorption of fat-soluble vitamins, and is a primary calorie source. Long chain fatty acids are needed for brain, retina, and nervous system development. They are deposited in the brain during the last trimester of pregnancy and are also found in breast milk.
Vitamins
The amount and types of vitamins in breast milk is directly related to the mother’s vitamin intake. This is why it is essential that she gets adequate nutrition, including vitamins. Fat-soluble vitamins, including vitamins A, D, E, and K, are all vital to the infant’s health. Water-soluble vitamins such as vitamin C, riboflavin, niacin, and panthothenic acid are also essential. Because of the need for these vitamins, many healthcare providers and lactation consultants will have nursing mothers continue on prenatal vitamins.
Carbohydrates
Lactose is the primary carbohydrate found in human milk. It accounts for approximately 40% of the total calories provided by breast milk. Lactose helps to decrease the amount of unhealthy bacteria in the stomach, which improves the absorption of calcium, phosphorus, and magnesium. It helps to fight disease and promotes the growth of healthy bacteria in the stomach.
Breast Milk is Best
Breast milk has the perfect combination of proteins, fats, vitamins, and carbohydrates. There is nothing better for the health of your baby. Leukocytes are living cells that are only found in breast milk. They help fight infection. It is the antibodies, living cells, enzymes, and hormones that make breast milk ideal. These cannot be added to formula.
Though some women ultimately are not able to breastfeed, many who think they cannot actually are able to breastfeed. Lactation consultants are able to provide support to women learning to breastfeed. For those who are not able to breastfeed, milk banks can be an alternative.
Last Updated: 08/2006
Compiled using information from the following sources:
Breastfeeding the Newborn: Clinical Strategies for Nurses. Biancuzzo, Marie, 1999.
Bestfeeding: How to Breastfeed Your Baby. Renfrew, Mary et al, 2004.
2.08.2010
Diaries of a Milk Maid
While pregnant with my first child I didn't have a strong belief or point of view on breastfeeding. It is widely accepted and believed to be the ideal choice of food for any infant, but for many, including my former self, formula is a perfectly acceptable substitute. Infant formulas are also often believed to be just as good as breastmilk. And why not believe this, it's how they are marketed, many hospital nurses push it even when you wish to breastfeed, and the answer to any problem with a nursing infant is to supplement with formula. Is it any wonder I hardly breastfed my first daughter past a few months?
During the short time I breastfed Maggie, I didn't enjoy it. I was told that cracked and bleeding nipples were part of the horrors of breastfeeding, and so when mine became cracked and bloody, I nursed through it, and of course, hated the experience. I wasn't informed by anyone that the choices I made, even in birth, could affect our nursing relationship or that just one bottle could be the beginning of the end. At that point in time, I don't know that having the information would have changed any of my choices anyway. For me, I think I had to take that path and make those choices. It has aided in the way I've formed my current opinions.
You see, I've been there, I've done that. I'm not looking down on women who were given poor advice or lack(ed) the information available. I didn't have it myself. I have been on all sides of the spectrum: I nursed and switched, I exclusively formula fed and I exclusively breastfed. When I say "I know how you feel" in regards to breastfeeding and formula feeding, I mean it.
Thankfully, despite not getting the best start in life, my girls are thriving and healthy. That's wonderful. I didn't see that and say to the indisputable scientific fact "This is untrue, my kids are FINE, therefore, formula does not decrease overall health!". No, instead I said, "This is amazing, interesting information. How lucky I am that my girls don't have (insert health issue, like asthma, diabetes, childhood obesity, etc) for not receiving breastmilk." But, just because my girls came out unscathed didn't mean I couldn't do my best to give my next baby an even better chance at a healthy start to his life. I made it my mission to succeed at breastfeeding. That mission started while I was pregnant with my son.
I read EVERYTHING. I joined breastfeeding forums to see what problems real women were facing with breastfeeding. I read "The Womanly Art of Breastfeeding" from cover to cover like it was the breastfeeding bible. I posted concerns and sought help, before I could even have a problem. I figured, the issues with breastfeeding in the past, for me, were all due to lack of information, so I armed myself. The worst thing, I imagined, would be to have an issue arrive, and try to find the answer at that time, rather than avoiding the issue to the best of my ability, or having the answer already.
I learned my nipples cracked and bled with my first daughter because she wasn't latched properly. A baby who's properly latched will not cause that kind of pain or damage. The only thing that should be expected is initial soreness, for the first few weeks and a slight discomfort at latch on. Once your baby is suckling away, it shouldn't hurt. If it does, it's not right. Learn about proper latch while pregnant. It's ok to have to "learn" to breastfeed. It's natural, but you and your baby will both have to be teachers and believers in each other.
I also learned that scheduling was not only unnecessary, but could hurt my supply and our nursing relationship. When you have a newborn, their stomach is only the size of a marble, and by 1 week the size of a pingpong ball. You cannot expect so much to fit in there. This is why your newborn will nurse almost constantly, because it can only take so much at a time. I didn't resent nursing every 1-2 hours, knowing this is what my baby needed and WHY he needed it.
Weight loss and weight gain are always on a parent's mind. Many babies will lose 10% of their birth weight while in the hospital. This is normal, I learned, and no cause for concern. I also found that when you're receiving IV fluids in labor, your baby is going to have water weight, so they aren't actually losing as much as you think. Wet and poopy diapers were the best way to gauge my newborn's intake, and there were definitely plenty of those!
I could write a book on this information (which is why La Leche League has done that with the womanly art of breastfeeding) because there is a solution or explanation to almost EVERY scenario in the breastfeeding world, you just have to know where to find that info!
If I had to limit my advice to the single most important factor in successful breastfeeding, it would be preemptive education/prevention. You don't search for the answers to the questions on your test while you're taking it, you prepare for it. You study, you perfect your knowledge the best you can with all the resources available. Breastfeeding should be no exception, if you truly wish to succeed. You'll find your breasts aren't too small or too large; that your baby may nurse every hour for 45 minutes or every 3 hours for 15; That your baby doesn't know how to latch right away and it may take 1 try or 100 tries. The one constant, the one truth, is that less than 3-5%(depending on the source) of women can truly not breastfeed their babies exclusively, so chances are, the issues you might be facing, can be worked through. You just need the tools.
During the short time I breastfed Maggie, I didn't enjoy it. I was told that cracked and bleeding nipples were part of the horrors of breastfeeding, and so when mine became cracked and bloody, I nursed through it, and of course, hated the experience. I wasn't informed by anyone that the choices I made, even in birth, could affect our nursing relationship or that just one bottle could be the beginning of the end. At that point in time, I don't know that having the information would have changed any of my choices anyway. For me, I think I had to take that path and make those choices. It has aided in the way I've formed my current opinions.
You see, I've been there, I've done that. I'm not looking down on women who were given poor advice or lack(ed) the information available. I didn't have it myself. I have been on all sides of the spectrum: I nursed and switched, I exclusively formula fed and I exclusively breastfed. When I say "I know how you feel" in regards to breastfeeding and formula feeding, I mean it.
Thankfully, despite not getting the best start in life, my girls are thriving and healthy. That's wonderful. I didn't see that and say to the indisputable scientific fact "This is untrue, my kids are FINE, therefore, formula does not decrease overall health!". No, instead I said, "This is amazing, interesting information. How lucky I am that my girls don't have (insert health issue, like asthma, diabetes, childhood obesity, etc) for not receiving breastmilk." But, just because my girls came out unscathed didn't mean I couldn't do my best to give my next baby an even better chance at a healthy start to his life. I made it my mission to succeed at breastfeeding. That mission started while I was pregnant with my son.
I read EVERYTHING. I joined breastfeeding forums to see what problems real women were facing with breastfeeding. I read "The Womanly Art of Breastfeeding" from cover to cover like it was the breastfeeding bible. I posted concerns and sought help, before I could even have a problem. I figured, the issues with breastfeeding in the past, for me, were all due to lack of information, so I armed myself. The worst thing, I imagined, would be to have an issue arrive, and try to find the answer at that time, rather than avoiding the issue to the best of my ability, or having the answer already.
I learned my nipples cracked and bled with my first daughter because she wasn't latched properly. A baby who's properly latched will not cause that kind of pain or damage. The only thing that should be expected is initial soreness, for the first few weeks and a slight discomfort at latch on. Once your baby is suckling away, it shouldn't hurt. If it does, it's not right. Learn about proper latch while pregnant. It's ok to have to "learn" to breastfeed. It's natural, but you and your baby will both have to be teachers and believers in each other.
I also learned that scheduling was not only unnecessary, but could hurt my supply and our nursing relationship. When you have a newborn, their stomach is only the size of a marble, and by 1 week the size of a pingpong ball. You cannot expect so much to fit in there. This is why your newborn will nurse almost constantly, because it can only take so much at a time. I didn't resent nursing every 1-2 hours, knowing this is what my baby needed and WHY he needed it.
Weight loss and weight gain are always on a parent's mind. Many babies will lose 10% of their birth weight while in the hospital. This is normal, I learned, and no cause for concern. I also found that when you're receiving IV fluids in labor, your baby is going to have water weight, so they aren't actually losing as much as you think. Wet and poopy diapers were the best way to gauge my newborn's intake, and there were definitely plenty of those!
I could write a book on this information (which is why La Leche League has done that with the womanly art of breastfeeding) because there is a solution or explanation to almost EVERY scenario in the breastfeeding world, you just have to know where to find that info!
If I had to limit my advice to the single most important factor in successful breastfeeding, it would be preemptive education/prevention. You don't search for the answers to the questions on your test while you're taking it, you prepare for it. You study, you perfect your knowledge the best you can with all the resources available. Breastfeeding should be no exception, if you truly wish to succeed. You'll find your breasts aren't too small or too large; that your baby may nurse every hour for 45 minutes or every 3 hours for 15; That your baby doesn't know how to latch right away and it may take 1 try or 100 tries. The one constant, the one truth, is that less than 3-5%(depending on the source) of women can truly not breastfeed their babies exclusively, so chances are, the issues you might be facing, can be worked through. You just need the tools.
2.05.2010
Dinosaur Vs. Bedtime
I saw this book at Target the other day and it immediately made me think of Alex. "Alex Vs. Bedtime" would be more appropriate, I thought. Last night was night #2 of him falling asleep without nursing. The night before was pretty hellish and he was up until almost midnight (not TOO uncommon for him) and he was NOT very happy. I just loved him and tried to snuggle with him. It was a battle, especially just trying to keep him contained on his little bed instead of running wildly around. Last night he was out by 11:30. From about 10-11 was pretty awful. But, around 11 he realized he wasn't going to get nursies until morning (even though we talked about and prepared for this and I repeated it over and over). He did say, in tears "Make me happy, mommy. Nursies make me happy.".
It was pretty heart breaking but I know that this is what is necessary for us at this point. I do not intend to wean Alex. I fully support him nursing until he's done, however, it's become more than an obsession and it's caused him to get little sleep, and me as well. I do not want the last part of our nursing relationship to be frustrating. I also do not want to resent his need to keep nursing, which is what I was beginning to feel.
I noticed in the last 2 nights that he actually stayed asleep longer before waking up asking to nurse. Night #1 he woke up frantic, flailing and screaming for it, but last night when he did finally stir, simply crawled into my bed and groggily asked to nurse. I let him. He also hasn't nursed at all today, and is currently napping. I do hope it doesn't lead to him weaning fully, I just want to cut down this night nursing...I cannot do it all night long, work part time, homeschool my older child and take care of them all day (and night, now that my husband works graveyards again).
So, tonight when it's time for Dinosaur to go to bed, I hope the roaring is down to a minimum and maybe we'll shave another 15 minutes off of that bedtime. He seemed to enjoy being sung to sleep last night, telling me "That's a good song, mom" after hearing "Twinkle, Twinkle" 3 times. :)
It was pretty heart breaking but I know that this is what is necessary for us at this point. I do not intend to wean Alex. I fully support him nursing until he's done, however, it's become more than an obsession and it's caused him to get little sleep, and me as well. I do not want the last part of our nursing relationship to be frustrating. I also do not want to resent his need to keep nursing, which is what I was beginning to feel.
I noticed in the last 2 nights that he actually stayed asleep longer before waking up asking to nurse. Night #1 he woke up frantic, flailing and screaming for it, but last night when he did finally stir, simply crawled into my bed and groggily asked to nurse. I let him. He also hasn't nursed at all today, and is currently napping. I do hope it doesn't lead to him weaning fully, I just want to cut down this night nursing...I cannot do it all night long, work part time, homeschool my older child and take care of them all day (and night, now that my husband works graveyards again).
So, tonight when it's time for Dinosaur to go to bed, I hope the roaring is down to a minimum and maybe we'll shave another 15 minutes off of that bedtime. He seemed to enjoy being sung to sleep last night, telling me "That's a good song, mom" after hearing "Twinkle, Twinkle" 3 times. :)
2.02.2010
Circumcision: The Uncut Version
I love this blogger. This particular article was so appreciated, though. It's just too bad that circumcision is still America's dirty little secret.
Sadly, many new parents do not even research circumcision. This is just as disappointing to me as when they choose to keep their sons intact, but do no research and therefore don't care properly for them. When we just blindly make decisions, especially those about our children's health (Vaccinations, elective surgeries, feeding, etc) we aren't just hurting ourselves, or our kids...but the population as a whole.
If you circumcise your son because it's "Just what everyone does" what other things are you going to alter in the name of popularity? Will you get your daughter a boob job in high school if "everyone else is doing it" according to rumor? Because that's all that myth is, a rumor. Roughly, only half of US boys are being circumcised today. In some areas, like the West Coast, that number is as low as 30%. But, I won't make an argument for something as important as circumcision based off of location. After all, perhaps you're on the East coast which boasts a disgustingly high circ rate of 90% in some areas. And after all, you may move someday.
I'd much rather convince you of the ill effects of infant circumcision with FACTS. To do so, I'm going to list common pros that are given in favor of circumcising young infant boys. Then, I'm going to explain why they're bull shit.
"My husband is circumcised, I don't want him to wonder why he doesn't look like daddy"
-This is a very common reason for wanting to circumcise an infant. But, let's just think about this for a second. What other body parts of your husband's need to match? If your son's ears are different, are you going to alter them? No. And hey, your son won't have the same genitalia as you, but you'll explain that to him, that boys and girls look different. So why not explain to him that his daddy had a surgery as a baby to remove his skin, but you didn't do that to him because *insert whatever reason here, like "You were born perfect".* I can tell you that your son, if he has any questions at all about dad's privates, will probably be more interested in why he has pubic hair and why daddy's penis is bigger than his. You don't go around performing elective surgeries on people so they match. We're all different and unique...this should involve a life lesson, not scalpels.
"All his peers will be circumcised and I don't want him teased in the locker room."
-If a child is going to be teased about something, there's little you can do to prevent it. He could be teased for having a small penis...you're not going to get it enlarged. Plus, this excuse works on the assumption that guys are going to be checking each other out in the locker room. In the rare event that someone were to poke fun at your kid for having a foreskin, there are many retorts your son could shoot back, like "Why are you checking out my junk, jealous?" or "At least I'm not lacking in that department and have my whole penis." There's no reason to alter your perfect infant because someday, someone in some random situation may tease him. Plus, I remind you that the circ rates are dropping, drastically. The boys of today are being left intact, much like the rest of the world (85% of the men in our world have their foreskins).
"Well, those two reasons aside, it's better for his health. It's cleaner, it's easier to clean and he won't spread STDs as easily."
-No, no, and, no. To understand this you have to first understand how the foreskin functions. In infant boys, the foreskin is fused to the glans (head of the penis) much like your finger nail is attached to your finger. When your baby pees, it flushes out the inner part of the foreskin (and remember that urine is sterile) so this works to keep your son clean. Also, by keeping his foreskin, you prevent feces from his diaper from touching his urethra or getting under his foreskin, and therefore, prevent the chance of him getting foreign bacteria in his urinary tract. Older studies suggested that circumcised boys were less likely to get UTIs. There are more studies that show no difference and others that show that intact boys get them less often. Regardless of what the truth is, girls are more prone to UTIs than either circumcised OR intact boys, and we treat them with proper hygiene and antibiotics, no surgery.
Now to clean, let's imagine this: An intact boy requires NO special care. Because the foreskin is fused to the glans, you do NOT retract it, ever. This could cause pain, tears, and adhesions. Instead, you wipe only what you see, like you wash your finger. If you circumcise your infant, you'll have much more to do. During the healing process, you'll be taking care of a wound, in a diaper. Afterward, you'll have to clean any skin that was still left very thoroughly so that he doesn't get an infection. You may also have to worry about the freshly cut skin trying to heal back to the glans, usually resulting in adhesions. Advice on this varies from "do not retract" (like in intact boys) to "you must retract to prevent the adhesions or break them" so there's really no TRUE information on what to do. When the intact boy retracts naturally (sometime between infancy and puberty, but most commonly toddlerhood) he can retract, rinse and replace at bathtime. No soaps, just water. No harder than if he lacked foreskin.
As far as STDs are concerned, no study really has the truth established. Those that say intact men are at greater risk, or rather carriers, of more infections (like HPV) are grossly incorrect and make little sense. The most commonly quoted study is about a group in Africa, where they taught the freshly circumcised men safe sex practices and provided them with condoms, but not the group they left intact. They also didn't factor that the freshly circumcised men weren't having sex while their penises healed. They found that the intact men contracted HIV more often than their cut counterparts, based on their poor approach of collecting this data. This study was, on top of it all, cut short (no pun intended). We can also look at the population of America and conclude this study makes no sense. Our own HIV/AIDS rate is quite high to that of other industrialized counter parts, yet, we have an astoundingly high circumcision rate (about 90% of grown men in the US are circumcised, as this was the rate about 20-some years ago). So, how is it that we have such a high rate of HIV/AIDS when we also have such a high rate of circumcision? That makes no sense...
On top of that, to argue in favor of surgery on infants, to possibly reduce the risk of STD transfer in adults is irresponsible. Instead, we need to teach our children how their bodies function, how STDs are transferred and contracted, and push safe sex. THIS is what will protect your son or daughter, not a false sense of protection because they were circumcised (or their partner is).
"But uncircumcised penises are soooo gross!"
-Really? How attractive is YOUR genitalia? If a man you were really in to took you home, and you started to fool around, and he caught a glimpse of your goods and never called you again because it was "so gross" he'd be labeled an asshole. Most genitals are not very attractive, female or male; circumcised or not. We are all made differently and none of us "match". To discount a person because they have foreskin is incredibly shallow. Just like a man discounting a woman for having an extended clitoris, longer labia, or not having her clitoral hood removed is shallow.
There is nothing gross about the state of a man's (or infant's) natural penis. This is how they are SUPPOSE to look; without tight skin or dark circle scars. We tend to be afraid of what we don't know, but that doesn't make it's ok. It's just ignorance to how a penis is suppose to look. If your son's toes were oddly shaped and ugly, you wouldn't remove them. They are part of him, and you love every bit.
"Well, I've never actually seen one. I didn't mean it was gross looking because of the skin, I meant because of all that nasty stuff that builds up in there!"
-If you've never seen one, how do you know it's nasty? Oh, because of rumors and stigmas surrounding intact men in America. Well, we're talking about infants, for one. Remember how I said the glans and foreskin were fused? Yea, there's nothing "building up". And, the "stuff" is called smegma. This is a natural lubricant produced by the body, you have it too. It's your discharge. It keeps your pH balance normal, it keeps you lubricated for sex, it keeps your skin there soft. Everyone needs to practice proper hygiene, circumcised men included. In the end, a dirty penis is a dirty penis. Most intact men take extra care to keep themselves clean, partly because there is such a stigma about having a foreskin. In order for smegma to build up, the man needs to really lack in caring for his man bits, and this would probably be no different if her were circumcised, and I doubt you'd put EITHER penises in your mouth. But again, we're talking about infants, and whether you need to worry about his for YOUR son...so again, the answer is no. For the first portion of his life, his foreskin is self cleaning, after that, you teach him how. After that, it's up to him whether he'll be a slob or a Mr. Clean kinda guy. Regardless, it's nothing to remove body parts over.
"If it was unnecessary, they wouldn't do it."
-Many insurance companies, and state medicaid, are no longer covering circumcisions. Certain hospitals have banned the procedure as well. I've heard, first hand from friends/aquaintances, quotes in the range of $350-$1500 to have the surgery performed on their newborn. The reasons given "It is not medically necessary, it is a preference." My co-worker and I were discussing this issue one day. She was telling me that she had taken him (her son) to the pediatrician to get it done, because the hospital didn't perform the. The pediatrician told her the procedure was not covered by her insurance because it was considered a cosmetic surgery, and it would cost them $400. She debated it, but he told her that there was absolutely no reason to do it, that many boys today aren't getting circumcised, and told her proper care (not to retract). He's 5 and while her intentions walking in to the pediatricians office that day were to circumcise him without a thought or any research, she told me how happy she is that it wasn't covered and that he remained intact. I'm pretty sure he'll be happy about that, too!
If there are any other reasons you've heard for someone wanting to circumcise, I'd love to hear them. If you've been considering it and are still confused, have more questions, etc I would love to address that.
There are so many decisions for new parents to make, and it's important that you're informed. What I found when researching circumcision was that EVERY pro-circ benefit could be debunked with medical facts. That was enough for me. Why expose my perfect newborn boy to the risks of bleeding, pain, MRSA staph infection, decreased sensitivity and genital integrity if there were no benefits to it?
For a great first time parent article, check this out: http://www.circumstitions.com/Itsaboy.html
Here's a group of doctors opposing circumcision: http://www.doctorsopposingcircumcision.org/
For a quick, easy fact-checking decision maker, look at this: http://circumcisiondecisionmaker.com/
To find out why this group is fighting for baby boy's rights, go here: http://www.intactamerica.org/
Already raising an intact son (or pregnant with one who'll stay that way) join us here:
*Raising Intact Boys* on cafemom.
Sadly, many new parents do not even research circumcision. This is just as disappointing to me as when they choose to keep their sons intact, but do no research and therefore don't care properly for them. When we just blindly make decisions, especially those about our children's health (Vaccinations, elective surgeries, feeding, etc) we aren't just hurting ourselves, or our kids...but the population as a whole.
If you circumcise your son because it's "Just what everyone does" what other things are you going to alter in the name of popularity? Will you get your daughter a boob job in high school if "everyone else is doing it" according to rumor? Because that's all that myth is, a rumor. Roughly, only half of US boys are being circumcised today. In some areas, like the West Coast, that number is as low as 30%. But, I won't make an argument for something as important as circumcision based off of location. After all, perhaps you're on the East coast which boasts a disgustingly high circ rate of 90% in some areas. And after all, you may move someday.
I'd much rather convince you of the ill effects of infant circumcision with FACTS. To do so, I'm going to list common pros that are given in favor of circumcising young infant boys. Then, I'm going to explain why they're bull shit.
"My husband is circumcised, I don't want him to wonder why he doesn't look like daddy"
-This is a very common reason for wanting to circumcise an infant. But, let's just think about this for a second. What other body parts of your husband's need to match? If your son's ears are different, are you going to alter them? No. And hey, your son won't have the same genitalia as you, but you'll explain that to him, that boys and girls look different. So why not explain to him that his daddy had a surgery as a baby to remove his skin, but you didn't do that to him because *insert whatever reason here, like "You were born perfect".* I can tell you that your son, if he has any questions at all about dad's privates, will probably be more interested in why he has pubic hair and why daddy's penis is bigger than his. You don't go around performing elective surgeries on people so they match. We're all different and unique...this should involve a life lesson, not scalpels.
"All his peers will be circumcised and I don't want him teased in the locker room."
-If a child is going to be teased about something, there's little you can do to prevent it. He could be teased for having a small penis...you're not going to get it enlarged. Plus, this excuse works on the assumption that guys are going to be checking each other out in the locker room. In the rare event that someone were to poke fun at your kid for having a foreskin, there are many retorts your son could shoot back, like "Why are you checking out my junk, jealous?" or "At least I'm not lacking in that department and have my whole penis." There's no reason to alter your perfect infant because someday, someone in some random situation may tease him. Plus, I remind you that the circ rates are dropping, drastically. The boys of today are being left intact, much like the rest of the world (85% of the men in our world have their foreskins).
"Well, those two reasons aside, it's better for his health. It's cleaner, it's easier to clean and he won't spread STDs as easily."
-No, no, and, no. To understand this you have to first understand how the foreskin functions. In infant boys, the foreskin is fused to the glans (head of the penis) much like your finger nail is attached to your finger. When your baby pees, it flushes out the inner part of the foreskin (and remember that urine is sterile) so this works to keep your son clean. Also, by keeping his foreskin, you prevent feces from his diaper from touching his urethra or getting under his foreskin, and therefore, prevent the chance of him getting foreign bacteria in his urinary tract. Older studies suggested that circumcised boys were less likely to get UTIs. There are more studies that show no difference and others that show that intact boys get them less often. Regardless of what the truth is, girls are more prone to UTIs than either circumcised OR intact boys, and we treat them with proper hygiene and antibiotics, no surgery.
Now to clean, let's imagine this: An intact boy requires NO special care. Because the foreskin is fused to the glans, you do NOT retract it, ever. This could cause pain, tears, and adhesions. Instead, you wipe only what you see, like you wash your finger. If you circumcise your infant, you'll have much more to do. During the healing process, you'll be taking care of a wound, in a diaper. Afterward, you'll have to clean any skin that was still left very thoroughly so that he doesn't get an infection. You may also have to worry about the freshly cut skin trying to heal back to the glans, usually resulting in adhesions. Advice on this varies from "do not retract" (like in intact boys) to "you must retract to prevent the adhesions or break them" so there's really no TRUE information on what to do. When the intact boy retracts naturally (sometime between infancy and puberty, but most commonly toddlerhood) he can retract, rinse and replace at bathtime. No soaps, just water. No harder than if he lacked foreskin.
As far as STDs are concerned, no study really has the truth established. Those that say intact men are at greater risk, or rather carriers, of more infections (like HPV) are grossly incorrect and make little sense. The most commonly quoted study is about a group in Africa, where they taught the freshly circumcised men safe sex practices and provided them with condoms, but not the group they left intact. They also didn't factor that the freshly circumcised men weren't having sex while their penises healed. They found that the intact men contracted HIV more often than their cut counterparts, based on their poor approach of collecting this data. This study was, on top of it all, cut short (no pun intended). We can also look at the population of America and conclude this study makes no sense. Our own HIV/AIDS rate is quite high to that of other industrialized counter parts, yet, we have an astoundingly high circumcision rate (about 90% of grown men in the US are circumcised, as this was the rate about 20-some years ago). So, how is it that we have such a high rate of HIV/AIDS when we also have such a high rate of circumcision? That makes no sense...
On top of that, to argue in favor of surgery on infants, to possibly reduce the risk of STD transfer in adults is irresponsible. Instead, we need to teach our children how their bodies function, how STDs are transferred and contracted, and push safe sex. THIS is what will protect your son or daughter, not a false sense of protection because they were circumcised (or their partner is).
"But uncircumcised penises are soooo gross!"
-Really? How attractive is YOUR genitalia? If a man you were really in to took you home, and you started to fool around, and he caught a glimpse of your goods and never called you again because it was "so gross" he'd be labeled an asshole. Most genitals are not very attractive, female or male; circumcised or not. We are all made differently and none of us "match". To discount a person because they have foreskin is incredibly shallow. Just like a man discounting a woman for having an extended clitoris, longer labia, or not having her clitoral hood removed is shallow.
There is nothing gross about the state of a man's (or infant's) natural penis. This is how they are SUPPOSE to look; without tight skin or dark circle scars. We tend to be afraid of what we don't know, but that doesn't make it's ok. It's just ignorance to how a penis is suppose to look. If your son's toes were oddly shaped and ugly, you wouldn't remove them. They are part of him, and you love every bit.
"Well, I've never actually seen one. I didn't mean it was gross looking because of the skin, I meant because of all that nasty stuff that builds up in there!"
-If you've never seen one, how do you know it's nasty? Oh, because of rumors and stigmas surrounding intact men in America. Well, we're talking about infants, for one. Remember how I said the glans and foreskin were fused? Yea, there's nothing "building up". And, the "stuff" is called smegma. This is a natural lubricant produced by the body, you have it too. It's your discharge. It keeps your pH balance normal, it keeps you lubricated for sex, it keeps your skin there soft. Everyone needs to practice proper hygiene, circumcised men included. In the end, a dirty penis is a dirty penis. Most intact men take extra care to keep themselves clean, partly because there is such a stigma about having a foreskin. In order for smegma to build up, the man needs to really lack in caring for his man bits, and this would probably be no different if her were circumcised, and I doubt you'd put EITHER penises in your mouth. But again, we're talking about infants, and whether you need to worry about his for YOUR son...so again, the answer is no. For the first portion of his life, his foreskin is self cleaning, after that, you teach him how. After that, it's up to him whether he'll be a slob or a Mr. Clean kinda guy. Regardless, it's nothing to remove body parts over.
"If it was unnecessary, they wouldn't do it."
-Many insurance companies, and state medicaid, are no longer covering circumcisions. Certain hospitals have banned the procedure as well. I've heard, first hand from friends/aquaintances, quotes in the range of $350-$1500 to have the surgery performed on their newborn. The reasons given "It is not medically necessary, it is a preference." My co-worker and I were discussing this issue one day. She was telling me that she had taken him (her son) to the pediatrician to get it done, because the hospital didn't perform the. The pediatrician told her the procedure was not covered by her insurance because it was considered a cosmetic surgery, and it would cost them $400. She debated it, but he told her that there was absolutely no reason to do it, that many boys today aren't getting circumcised, and told her proper care (not to retract). He's 5 and while her intentions walking in to the pediatricians office that day were to circumcise him without a thought or any research, she told me how happy she is that it wasn't covered and that he remained intact. I'm pretty sure he'll be happy about that, too!
If there are any other reasons you've heard for someone wanting to circumcise, I'd love to hear them. If you've been considering it and are still confused, have more questions, etc I would love to address that.
There are so many decisions for new parents to make, and it's important that you're informed. What I found when researching circumcision was that EVERY pro-circ benefit could be debunked with medical facts. That was enough for me. Why expose my perfect newborn boy to the risks of bleeding, pain, MRSA staph infection, decreased sensitivity and genital integrity if there were no benefits to it?
For a great first time parent article, check this out: http://www.circumstitions.com/Itsaboy.html
Here's a group of doctors opposing circumcision: http://www.doctorsopposingcircumcision.org/
For a quick, easy fact-checking decision maker, look at this: http://circumcisiondecisionmaker.com/
To find out why this group is fighting for baby boy's rights, go here: http://www.intactamerica.org/
Already raising an intact son (or pregnant with one who'll stay that way) join us here:
*Raising Intact Boys* on cafemom.
1.29.2010
Rules and Regulations: As They Pertain to Nursing Toddlers
So after working a short closing shift at the store tonight, I came home to a sleepy Alex who wanted mama snuggles. I welcomed him with open arms but attempted to put off the insistent "nursies" requests. You see, while I strongly believe in child-led weaning, we are at a point where I must set limits. The nursing relationship should continue so long as both parties are happy with it. I wasn't happy where we were at but I figured there was a happy medium between nursing CONSTANTLY at 2 years old, and weaning completely.
So, I've implemented a few "rules" for our nursing time. This is for both of our sanity. Mine, so that I don't resent the nursing relationship and can enjoy it until it naturally ends and him so that I don't loose my mind! HAHA
That being said, I never saw myself setting limits on nursing behavior. I figured that in the first year I would nurse 100% on demand with the exception of certain rare circumstances; and I did. After the first year, I continued to allow him free access at all times, but as he grew a little older I noticed that instead of nursing less at night and gradually dropping night feedings, he was nursing ALL night. After observing and taking some time to think about what was going on, I realized that he was such a busy toddler during the day (playing, rough housing, etc) that he was literally too busy for nursies. Here he was burning all this energy and then making up for it at night. Now of course, I always offered him a full course of meals throughout the day, but he was not too big on eating, still isn't that big of an eater.
This was where I started to question natural full-term nursing, maybe it wasn't for us. But, I kept reminding myself that there had to be a way to make it work, I was going to give it that minimum 2 years. Perhaps part of my drive to continue nursing was subconciously due to not nursing my other 2 children. Nonetheless, I wasn't going to call it quits without putting forth some effort.
So, at around 16 months I tried to offer him to nurse more during the day, hoping this would decrease those night time feedings. That proved unsuccessful. I ended up nursing more during the day, and just as much at night. Can we say "ouch"?
The next course of action was to try other methods of getting him back to sleep when he stirred. It makes sense, it's a logical choice. So I'd pat him and rock him, and he'd cry for nursies. I'd have my husband try to soothe him, and he'd cry for nursies. Now, you'd think that after just a few minutes of being loved and cuddled and crying he'd go back to sleep. No. This kid could literally scream for hours for nursies. Oye. After a few nights, my husband and I could not take it and we gave in to the nursies.
It seemed to let up a little, he wasn't attached literally all night long. I could live with a few night time feedings. However, out of nowhere it seemed to start up again, this time he was almost 20 months old. I couldn't stand it. Like I said, I was beginning to resent nursing, as a whole, because the night time nursing seemed so out of hand. But I couldn't let him scream all night either, I have 2 other children to take care of in the day and need to sleep!
My local La Leche League had some good tips: Talk about how nursies go to sleep at night and he can have them when the sun comes up, refuse a few times and put it off before giving in, keep doing what we were doing and within a week or two he should get it, etc. Ok, great. New game plan, let's do it!
I talked to him about how the nursies have to go to sleep as well and then when the sun comes up, they are awake again and he can have them. He liked to talk about this and we showed him the sun through the blinds and kept watching as it set, then we'd exclaim "Bed time, nursies!" and let him nurse one last time. This ended up not working too well. I could put him off a little in the middle of the night, for the first few wakings, but by 4am he wanted them, no questions asked.
This has been an ongoing battle and we've at least gotten it to the point that he's not nursing all night long, only a few times to fall back asleep. We lay him to sleep in his little bed after he's fallen asleep and he comes joining us that first time he wakes up, I just wish I knew how to keep him asleep all night...perhaps it's an unreasonable expectation. Maybe he inherited my poor sleeping habits. It might be due, now, to the fact that I am working part time away from the home. Whatever it is, it's one of the ongoing battles we face as parents. I *know* that nursing him longer will provide better health now and over all for the rest of his life. It's not that I mind, regardless of the difference in opinion of many peers and even family members. The science can't be argued because of personal opinions and comfort. For Alex and myself, it's just something we have to work on, much like a biting face or pants wetting.
After all, I'm sure I'll get a good night's sleep in about 18 years...right?
(Ironically enough, I stumbled upon this shortly after writing this blog. Hmm.)
So, I've implemented a few "rules" for our nursing time. This is for both of our sanity. Mine, so that I don't resent the nursing relationship and can enjoy it until it naturally ends and him so that I don't loose my mind! HAHA
That being said, I never saw myself setting limits on nursing behavior. I figured that in the first year I would nurse 100% on demand with the exception of certain rare circumstances; and I did. After the first year, I continued to allow him free access at all times, but as he grew a little older I noticed that instead of nursing less at night and gradually dropping night feedings, he was nursing ALL night. After observing and taking some time to think about what was going on, I realized that he was such a busy toddler during the day (playing, rough housing, etc) that he was literally too busy for nursies. Here he was burning all this energy and then making up for it at night. Now of course, I always offered him a full course of meals throughout the day, but he was not too big on eating, still isn't that big of an eater.
This was where I started to question natural full-term nursing, maybe it wasn't for us. But, I kept reminding myself that there had to be a way to make it work, I was going to give it that minimum 2 years. Perhaps part of my drive to continue nursing was subconciously due to not nursing my other 2 children. Nonetheless, I wasn't going to call it quits without putting forth some effort.
So, at around 16 months I tried to offer him to nurse more during the day, hoping this would decrease those night time feedings. That proved unsuccessful. I ended up nursing more during the day, and just as much at night. Can we say "ouch"?
The next course of action was to try other methods of getting him back to sleep when he stirred. It makes sense, it's a logical choice. So I'd pat him and rock him, and he'd cry for nursies. I'd have my husband try to soothe him, and he'd cry for nursies. Now, you'd think that after just a few minutes of being loved and cuddled and crying he'd go back to sleep. No. This kid could literally scream for hours for nursies. Oye. After a few nights, my husband and I could not take it and we gave in to the nursies.
It seemed to let up a little, he wasn't attached literally all night long. I could live with a few night time feedings. However, out of nowhere it seemed to start up again, this time he was almost 20 months old. I couldn't stand it. Like I said, I was beginning to resent nursing, as a whole, because the night time nursing seemed so out of hand. But I couldn't let him scream all night either, I have 2 other children to take care of in the day and need to sleep!
My local La Leche League had some good tips: Talk about how nursies go to sleep at night and he can have them when the sun comes up, refuse a few times and put it off before giving in, keep doing what we were doing and within a week or two he should get it, etc. Ok, great. New game plan, let's do it!
I talked to him about how the nursies have to go to sleep as well and then when the sun comes up, they are awake again and he can have them. He liked to talk about this and we showed him the sun through the blinds and kept watching as it set, then we'd exclaim "Bed time, nursies!" and let him nurse one last time. This ended up not working too well. I could put him off a little in the middle of the night, for the first few wakings, but by 4am he wanted them, no questions asked.
This has been an ongoing battle and we've at least gotten it to the point that he's not nursing all night long, only a few times to fall back asleep. We lay him to sleep in his little bed after he's fallen asleep and he comes joining us that first time he wakes up, I just wish I knew how to keep him asleep all night...perhaps it's an unreasonable expectation. Maybe he inherited my poor sleeping habits. It might be due, now, to the fact that I am working part time away from the home. Whatever it is, it's one of the ongoing battles we face as parents. I *know* that nursing him longer will provide better health now and over all for the rest of his life. It's not that I mind, regardless of the difference in opinion of many peers and even family members. The science can't be argued because of personal opinions and comfort. For Alex and myself, it's just something we have to work on, much like a biting face or pants wetting.
After all, I'm sure I'll get a good night's sleep in about 18 years...right?
(Ironically enough, I stumbled upon this shortly after writing this blog. Hmm.)
Subscribe to:
Posts (Atom)







